Why Do Babies Wear Helmets? Understanding Plagiocephaly Treatment & More
Have you ever strolled through a park or a shopping mall and spotted an infant with a sleek, custom-fitted helmet that looks more like futuristic headgear than a baby accessory? Your immediate thought is likely the one millions of parents have had: why do babies wear helmets? This sight can spark a wave of curiosity and, for new or expecting parents, a touch of concern. Is it for protection? Is it a medical necessity? The answer is a fascinating journey into infant development, pediatric medicine, and proactive parenting. These helmets, formally known as cranial orthoses, are not for safety from falls but are a prescribed medical device used to treat a condition called positional plagiocephaly, commonly known as flat head syndrome. This comprehensive guide will walk you through everything you need to know—from the science behind the condition to the realities of helmet therapy, empowering you with knowledge and dispelling common myths.
Understanding Positional Plagiocephaly: The "Why" Behind the Helmet
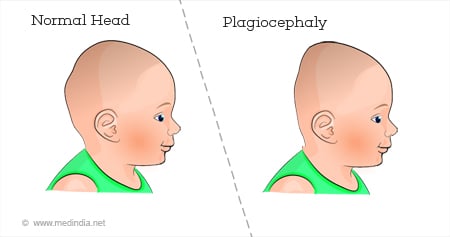
To truly understand why babies wear helmets, we must first grasp the condition they treat. Positional plagiocephaly is the medical term for a persistent, uneven flattening of an infant's skull. It's crucial to distinguish this from craniosynostosis, a more serious condition where the skull bones fuse prematurely, which often requires complex surgery. Positional plagiocephaly, by contrast, is almost always a positional issue, meaning it develops from external pressure on a soft, malleable infant skull.
The Perfect Storm: How Flat Head Syndrome Develops
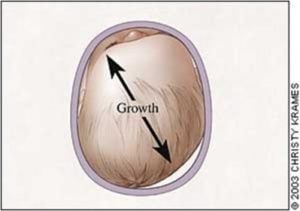
An infant's skull is a marvel of biological engineering. Composed of several soft plates separated by sutures and fontanelles (soft spots), this design allows the brain to grow rapidly and facilitates a safer passage through the birth canal. This same softness, however, makes the skull susceptible to molding. The "Back to Sleep" campaign, launched by the American Academy of Pediatrics (AAP) in 1994, is a monumental public health success story that dramatically reduced the incidence of Sudden Infant Death Syndrome (SIDS) by advocating for infants to sleep on their backs. This life-saving practice, while essential, created a new, less common challenge: prolonged pressure on the back or one side of the head. When babies spend extensive time lying in the same position—in cribs, car seats, bouncers, or swings—their skull can gradually flatten in that area. Torticollis, a tightening of the neck muscles that makes a baby prefer turning their head to one side, is a frequent companion to plagiocephaly, as the baby cannot easily reposition their head to relieve pressure.
Key Contributing Factors:
- Sleep Position: As mentioned, supine (back) sleeping is the primary safe sleep recommendation, but it increases pressure on the occiput (back of the head).
- Torticollis: A tight neck muscle limits head movement, causing the baby to consistently rest on the same spot.
- Prematurity: Premature babies have even softer skulls and often spend initial weeks in NICU beds with their heads in a fixed position.
- Multiple Births: Confined space in utero can lead to initial head shaping.
- Lack of "Tummy Time": Supervised awake time on the stomach is critical for strengthening neck and shoulder muscles and taking pressure off the back of the head.
Helmet Therapy Explained: The Corrective Power of Cranial Orthoses
When repositioning strategies and physical therapy for torticollis aren't sufficient to correct the flattening by around 4-6 months of age, a pediatrician or pediatric neurosurgeon/plastic surgeon may recommend helmet therapy. This brings us to the core of why babies wear helmets: to gently, painlessly, and permanently redirect the skull's growth.
How Do Baby Helmets Actually Work?
Think of the helmet not as a mold that crushes the head, but as a dynamic growth guide. The custom-made helmet is engineered with a soft, foam interior and a hard, plastic shell. It is precisely crafted from a 3D scan or plaster cast of the baby's head to have a void—a space—directly over the flattened area. The helmet's design applies gentle, constant pressure on the prominent, protruding parts of the skull while providing a void for the flat spot to grow into. The human skull is not solid bone; it has sutures that allow for growth. The helmet harnesses this natural growth potential. As the baby's brain grows (it reaches about 80% of its adult size by age 2!), the skull naturally expands. The helmet guides this expansion, encouraging more growth in the flattened area and restraining growth in the prominent areas, gradually creating a more symmetrical, round head shape over time.
Key Takeaway: The helmet does not squeeze the baby's head. It creates a pathway for natural growth. The pressure applied is minimal—often described as the pressure you feel when wearing a tight baseball cap—and is completely painless. Babies typically adapt within a few days.
The Helmet Therapy Journey: What to Expect
For parents facing this recommendation, the process can seem daunting. Understanding the typical timeline demystifies the experience.
Evaluation & Prescription: The process begins with a thorough examination by a specialist. They use a 3D scanner (like a handheld iPad-like device) to create a precise digital model of the baby's head. This scan is analyzed with specialized software that calculates the asymmetry, volume difference, and cephalic index (a measure of head width vs. length). A prescription is written if the asymmetry meets clinical thresholds (often a cranial vault asymmetry (CVA) of 5-7mm or more).
Casting/Scanning & Fabrication: The specialist's office takes the 3D scan. This digital file is sent to a lab where technicians design and 3D-print or carve a custom helmet. The entire process from scan to helmet delivery usually takes 2-3 weeks.
Fitting & "Break-In" Period: The first helmet fitting is a milestone. The orthotist (the specialist who fits the helmet) ensures a perfect fit—snug but not tight, with the correct amount of space over the flat area. There is a "break-in" period of 5-7 days where the baby wears the helmet for only a few hours a day to acclimate. Parents are taught how to check for redness (a normal, temporary sign of pressure) and how to clean the helmet.
Wearing Schedule & Monitoring: The standard protocol is 23 hours a day, with removal only for bathing and brief periods of supervised play without the helmet. Regular follow-up appointments (every 2-4 weeks) are critical. At each visit, the orthotist checks the fit, assesses progress via new scans, and may make minor adjustments by grinding down the foam interior to accommodate growth or changing the pressure points. Treatment duration varies but averages 3-6 months, depending on the baby's age at start and severity of the asymmetry.
Weaning & Completion: Once the desired symmetry is achieved (often when the baby is 12-18 months old, as the skull bones begin to harden), the weaning process begins. The baby will wear the helmet for fewer hours each day over 2-4 weeks to allow the skull to settle into its new shape without the device's guidance. The final scan is then compared to the initial one to showcase the remarkable correction.
Addressing Common Concerns and Questions
When parents first see why babies wear helmets, a flood of questions arises. Let's address the most pressing ones head-on.
Is Helmet Therapy Painful or Uncomfortable for My Baby?
No. The vast majority of babies adapt quickly. The initial few days might involve some fussiness as they feel the new sensation, but it is not painful. Any redness that appears is a normal, temporary sign of gentle pressure and fades within 20 minutes of helmet removal. The helmet is well-ventilated and lightweight. Parents often report their babies barely notice it after the first week, crawling, playing, and sleeping peacefully.
Are Helmets Purely Cosmetic? Is Treatment Really Necessary?
This is the most critical question. No, it is not purely cosmetic. While a symmetrical head shape is the visible outcome, the primary goals are functional and neurological:
- Optimal Brain Growth: The helmet ensures the skull has adequate, symmetrical volume to accommodate the growing brain without restriction.
- Facial Symmetry: Significant plagiocephaly can lead to asymmetry in the face, including the ears, eyes, and jaw. Correcting head shape early promotes balanced facial development.
- Potential Long-Term Issues: While research is ongoing, some studies suggest a correlation between moderate to severe untreated plagiocephaly and later issues like temporomandibular joint (TMJ) problems, visual field deficits, and even subtle neurodevelopmental delays. Early correction is a proactive measure for holistic development.
- Psychosocial Factors: As children grow, a noticeable head asymmetry can lead to teasing, self-esteem issues, and bullying. Early treatment prevents this future social challenge.
What Are the Alternatives or Complementary Strategies?
Helmets are not the first line of defense. Prevention and early intervention are paramount. From birth, pediatricians should assess head shape at every well-baby visit. The following strategies are foundational:
- Aggressive Tummy Time: Start from day one. Aim for multiple short sessions daily, building up to 30+ minutes total by 3 months. This is the single most effective preventative measure.
- Repositioning: Alternate the direction you lay your baby in the crib (so they turn their head to look out, not always toward the room). Switch which arm you hold them in during feedings. Encourage them to turn to the less-preferred side during play by placing toys, mirrors, or your face on that side.
- Physical Therapy: If torticollis is diagnosed, a pediatric physical therapist will provide specific stretches and exercises to loosen the tight neck muscle and strengthen the opposite side. This is almost always done in conjunction with helmet therapy if a helmet is needed.
- Specialty Pillows & Mattresses: While not a substitute for the above, some products (like the "Boppy" for tummy time support or specialized sleep surfaces with cut-outs) can be helpful tools under supervision. Always follow safe sleep guidelines: no loose items or pillows in the crib with a sleeping infant.
The Bigger Picture: Statistics, Safety, and Success
Understanding the prevalence and outcomes helps contextualize the decision.
- Prevalence: Positional plagiocephaly is surprisingly common. Studies suggest that up to 48% of infants have some degree of head flattening by 2 months of age, though most mild cases resolve with repositioning. The need for helmet therapy is estimated at 1 in 300 to 1 in 60 infants, with rates increasing since the "Back to Sleep" campaign.
- Timing is Everything: Treatment is most effective when started between 4 and 12 months of age. This is the peak growth period for the skull, and the sutures are still very flexible. Starting after 18 months is less effective and may require much longer treatment times.
- Success Rates: When fitted correctly and worn as prescribed, helmet therapy boasts over 90% success rates in achieving significant cosmetic and volumetric correction. The results are permanent.
- Safety: Modern cranial orthoses are regulated medical devices (FDA-cleared in the US). They are made from medical-grade, hypoallergenic, breathable materials. Serious complications are extremely rare when managed by a certified orthotist and pediatric team.
Making the Decision: A Partnership with Your Pediatric Team
Choosing helmet therapy is a significant decision. It involves a financial commitment, a time commitment, and an emotional adjustment to seeing your baby in a device. However, it is a decision made from a place of proactive care. The process is a collaborative effort between you, your pediatrician, a pediatric specialist (neurosurgeon, plastic surgeon, or orthotist), and often a physical therapist.
Actionable Steps for Parents:
- Be Proactive: At every well-baby check, ask your pediatrician about your baby's head shape. Don't wait for them to bring it up.
- Seek a Specialist: If a concern is raised, get a referral to a board-certified pediatric orthotist or a pediatric craniofacial team. They have the specific training and technology for diagnosis and treatment.
- Ask Questions: At the consultation, ask about the specific measurements (CVA, cephalic index), the expected treatment duration, the follow-up schedule, and the provider's experience and success rates.
- Connect with Other Parents: Many orthotist offices can connect you with families who have gone through treatment. Hearing firsthand experiences can be incredibly reassuring.
- Focus on the Goal: Remind yourself that this is a temporary measure for a permanent, positive outcome. The months of helmet wear are a small investment in your child's long-term health and confidence.
Conclusion: A Symbol of Proactive Care, Not Cause for Alarm
So, why do babies wear helmets? They wear them because modern medicine has provided a safe, effective, and non-invasive solution to a common developmental challenge. It is a testament to vigilant pediatric care and informed parenting. These sleek devices are not a sign of something "wrong" with a baby, but rather a proactive tool used to guide natural growth toward optimal symmetry and function. The next time you see a baby in a helmet, you'll know it's not for protection from the world, but a gentle guide shaping a healthier future. If you have concerns about your baby's head shape, speak with your pediatrician. Early detection and intervention are the keys to the simplest, most successful outcome, ensuring your little one can grow, learn, and explore the world with a head that is as perfectly formed as their bright, curious mind.