How Much Crown Visibility Is Normal? Your Complete Guide To Understanding Hair Thinning
Have you ever caught your reflection in a mirror or a photo and wondered, "Is that more scalp I'm seeing at the back of my head?" That moment of uncertainty is more common than you think. The concern about crown visibility—the amount of scalp showing through the hair at the vertex, or the top-back part of your head—plagues millions of people worldwide. It’s a subtle change that can spark significant anxiety, but the truth is, some degree of crown visibility is entirely normal and varies dramatically from person to person. So, how much crown visibility is normal? The answer isn't a simple measurement; it's a nuanced understanding of your personal hair pattern, age, genetics, and overall health. This comprehensive guide will decode the mystery of crown visibility, helping you distinguish between natural variation and potential signs of hair loss, and empowering you with actionable knowledge and solutions.
Understanding the Crown: Anatomy and What "Visibility" Really Means
Before we can define "normal," we need to understand the landscape. The crown, or vertex, is the rounded area at the top-back of the skull. It's a common site for pattern hair loss (androgenetic alopecia) because hair follicles in this region are often more sensitive to hormonal changes, particularly dihydrotestosterone (DHT). Crown visibility refers to the degree to which the scalp is seen through the hair in this area. It's not just about a bald spot; it's about the overall hair density and part width.
Hair density is measured in hairs per square centimeter. A "normal" density can range from 150 to 200+ hairs/cm². However, what you see is also affected by:
- Hair caliber: Thicker hair strands provide more coverage than fine, vellus-like hairs.
- Hair color contrast: Dark hair on light skin creates more obvious contrast than light hair on light skin.
- Hair texture and curl: Curly or wavy hair can create an illusion of greater volume and density compared to straight, fine hair.
- Hair parting style: How you naturally part your hair can either minimize or accentuate the crown.
Therefore, crown visibility is a visual assessment of the interplay between hair density, strand characteristics, and scalp pigmentation. It’s a spectrum, not a binary state of "covered" or "bald."
What is Considered "Normal" Crown Visibility? It Depends.
This is the core of your question. There is no single, universal standard for "normal" crown visibility. What’s normal for a 25-year-old with thick, dark, curly hair is vastly different from what’s normal for a 65-year-old with fine, gray, straight hair. Let's break down the key factors.
Normal Variation by Age and Gender
Hair naturally thins with age for nearly everyone. This is called senile alopecia or age-related hair miniaturization.
- In Men: By age 30, about 25% show some signs of male pattern baldness (MPB), often starting with a subtle increase in crown visibility or a receding hairline. By 50, roughly 50% have significant hair loss, with the crown frequently involved. A slightly widened part or a small, stable "bald spot" the size of a coin that hasn't changed in years can be a normal part of aging for many men.
- In Women: Female pattern hair loss (FPHL) typically presents as diffuse thinning over the crown while the frontal hairline remains intact. It's less about a bald spot and more about a widening part and reduced volume. About 40% of women will experience some degree of FPHL by age 50. A moderate increase in scalp visibility at the crown, especially when hair is parted down the middle, is a common and often normal age-related change.
Normal Variation by Ethnicity and Hair Type
- Hair Texture: Individuals with very fine, straight hair (common in East Asian and some Caucasian populations) will naturally show more scalp visibility than those with coarse, curly, or kinky hair (common in African and Afro-Caribbean populations), even at identical densities. The curl creates physical volume and shadow that hides the scalp.
- Hair Color: The contrast between hair and scalp color is critical. A person with jet-black hair and pale skin will have dramatically more obvious crown visibility at a given density than someone with medium-brown hair and olive skin.
- Hair Density by Ethnicity: Baseline genetic hair density can vary. Some studies suggest individuals of African descent may have lower average hair density but higher hair diameter, while those of East Asian descent may have higher density but lower diameter. The net visual effect is what matters.
Key Takeaway:Normal is personal. Your "normal" baseline is what you had in your late teens/early twenties, adjusted for the natural, gradual thinning that comes with aging. A sudden, noticeable increase in visibility is what warrants attention.
When Does Crown Visibility Become a Red Flag? Signs of Abnormal Loss
While some visibility is normal, a rapid or progressive increase is not. Here are the key signs that your crown visibility may indicate active, problematic hair loss:
- Accelerated Change: You notice a significant difference in crown visibility over the past 6-12 months. Photos from a year ago show noticeably more hair.
- The "U-Shaped" or "O-Shaped" Pattern: In men, the classic sign of androgenetic alopecia is a bald spot that starts at the crown and may eventually meet a receding hairline, forming a "horseshoe" pattern. In women, it's a preserved frontal hairline with widening part and diffuse thinning at the crown.
- Excessive Shedding: You're finding more than 100 hairs per day on your pillow, in the shower, or on your brush. While shedding is normal (50-100 hairs/day), a sustained increase is a major red flag.
- Scalp Changes: The skin at the crown becomes noticeably more shiny, tight, or wrinkled. This indicates significant follicle loss and skin atrophy.
- Miniaturized Hairs: If you look closely at the thinning area, you see many short, fine, wispy hairs (vellus hairs) that never seem to grow long. These are miniaturized follicles, a hallmark of genetic pattern loss.
- Itching, Pain, or Inflammation: Hair loss accompanied by an itchy, flaky, red, or painful scalp suggests an inflammatory or autoimmune condition like alopecia areata, lichen planopilaris, or severe seborrheic dermatitis.
If you identify with one or more of these signs, especially accelerated change or a classic pattern, it's time to investigate further.
The Usual Suspects: Common Causes of Excessive Crown Visibility
Understanding the "why" is crucial for finding the right solution. Excessive crown visibility is a symptom, not a diagnosis.
1. Androgenetic Alopecia (Pattern Hair Loss)
This is the most common cause, affecting over 50 million men and 30 million women in the U.S. alone. It's genetically programmed and hormonally driven.
- Mechanism: DHT (a derivative of testosterone) binds to susceptible follicles, miniaturizing them over cycles. The crown and temples are classic "DHT-sensitive" zones.
- Pattern: Men: Vertex balding. Women: Diffuse crown thinning.
- Progression: It's chronic and progressive without intervention. Early treatment is key to preserving existing hair.
2. Telogen Effluvium (TE) - The Shedding Disorder
This is a reactive, non-scarring hair loss triggered by a systemic shock to the body.
- Triggers: Severe stress, major surgery, childbirth, rapid weight loss, extreme diets, serious illness (e.g., COVID-19), or certain medications.
- Mechanism: A large number of hairs are pushed prematurely into the shedding (telogen) phase. 2-3 months later, diffuse shedding occurs. The crown can be hit hard because it's often already the weakest point.
- Key Point: TE itself doesn't cause permanent baldness, but it can unmask underlying androgenetic alopecia. If you have a genetic predisposition, a TE episode can accelerate crown thinning.
3. Traction Alopecia
This is mechanical damage from constant tension on hair follicles.
- Causes: Tight hairstyles like ponytails, buns, braids, weaves, or extensions. Frequent use of headbands or hats that pull.
- Pattern: Often starts at the hairline and temples, but can affect the crown if hairstyles put tension there (e.g., tight top knots).
- Reversibility: Early stages are reversible if the tension is stopped. Chronic traction leads to permanent follicle damage.
4. Nutritional Deficiencies & Medical Conditions
Hair follicles are metabolically active. Deficiencies can stunt growth.
- Key Nutrients: Iron (especially in women), vitamin D, B vitamins (biotin, B12), zinc, protein.
- Medical Conditions: Thyroid disorders (hypo- or hyperthyroidism), autoimmune diseases (lupus), anemia, and scalp infections like tinea capitis (ringworm).
- Note: Deficiencies usually cause diffuse shedding (like TE), not a patterned bald spot, but can worsen existing crown thinning.
5. Scalp Conditions
Inflammation and damage to the scalp environment harm follicles.
- Seborrheic Dermatitis & Psoriasis: Flaky, itchy, inflamed scalp. Chronic inflammation can lead to hair loss.
- Folliculitis Decalvans: A rare, scarring bacterial inflammation that destroys follicles, causing permanent bald patches.
How to Honestly Assess Your Crown Visibility: A Step-by-Step Guide
Self-assessment is the first step. Be objective and consistent.
- Use Consistent Lighting and Tools: Assess your crown in bright, natural daylight or a well-lit bathroom. Use a handheld mirror or ask someone to take a clear photo from directly above.
- The "Part Test": Part your hair in the center and on both sides. Look at the width of the part at the crown. Is it wider than it used to be? A widening part is a classic sign of diffuse thinning.
- The "Comb-Through" Test: Gently comb your hair forward from the crown towards your forehead. Do you see more scalp between the hairs? Is the hair at the crown significantly shorter or finer than hair at the sides and back?
- The "Flash Test": Take a photo with a camera flash directly on the crown. The flash will illuminate any translucent areas, making scalp visibility starkly obvious.
- Track Over Time: Take standardized photos (same lighting, same part, same distance) every 3-6 months. This is the best way to detect progressive change, which is the true indicator of active loss.
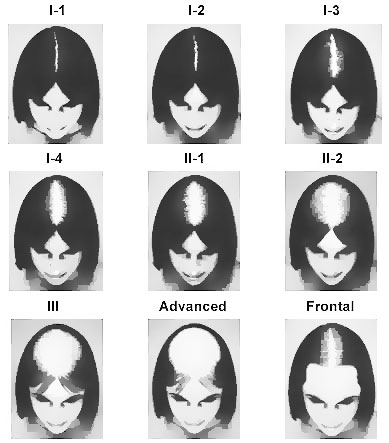
- Consider the "Hair Coverage Index": Dermatologists sometimes use a scale like the Savin Scale for women or the Hamilton-Norwood Scale for men. Familiarize yourself with these to roughly categorize your pattern.
Remember: Self-diagnosis has limits. If you're concerned, a professional evaluation is essential.
Solutions and Strategies: What You Can Do About Crown Visibility
Treatment depends entirely on the cause. Here’s a breakdown of evidence-based options.
Medical Treatments (FDA-Approved & Off-Label)
- Minoxidil (Rogaine): A topical (and sometimes oral) vasodilator. It's a growth stimulant, not a DHT blocker. It's most effective for vertex (crown) balding in men and diffuse thinning in women. Consistency is critical; you must apply it twice daily, indefinitely. Shedding is common in the first 1-3 months.
- Finasteride (Propecia): An oral prescription drug that inhibits the conversion of testosterone to DHT. It's highly effective at halting progression and regrowing hair in the crown for men. Not approved for women of childbearing age due to birth defect risks. Requires a prescription and monitoring for side effects (rare but possible).
- Spironolactone: An anti-androgen prescription for women with FPHL. It blocks androgen receptors and reduces androgen production.
- Low-Level Laser Therapy (LLLT): Devices like laser combs/helmets use red light to stimulate cellular activity in follicles. Evidence is moderate but promising, often used as an adjunct to other treatments.
- Platelet-Rich Plasma (PRP): Injections of your own concentrated platelets into the scalp to promote healing and growth. Shows good results for many, especially in early-stage crown thinning, but is costly and requires multiple sessions.
Cosmetic and Surgical Solutions
- Hair Transplant Surgery:Follicular Unit Extraction (FUE) or Follicular Unit Transplantation (FUT). Healthy follicles from the dense donor area (back and sides of head) are harvested and implanted into the thinning crown. It's a redistribution, not a cure for ongoing loss. You must be on medical therapy (minoxidil/finasteride) to protect your native hair post-transplant.
- Scalp Micropigmentation (SMP): A cosmetic tattoo technique that deposits pigment into the scalp to create the illusion of density. It's excellent for shaved heads or to camouflage a thinning crown after a transplant or as an alternative. It's a permanent makeup procedure.
- Hair Fibers and Sprays: Cosmetic powders (e.g., Toppik, Caboki) that cling to existing hair and scalp to create an instant appearance of thickness. They wash out with shampoo. A great short-term solution.
Lifestyle and Supportive Measures
- Nutrition: Ensure a balanced diet rich in protein, iron, zinc, and vitamins. Consider a supplement if deficient (get tested first).
- Stress Management: Chronic stress elevates cortisol, which can disrupt hair growth cycles. Practice mindfulness, exercise, adequate sleep.
- Gentle Hair Care: Avoid tight hairstyles, harsh chemical treatments, and excessive heat. Use a wide-tooth comb, avoid vigorous towel-drying.
- Scalp Health: Use a gentle, anti-dandruff shampoo (with ketoconazole, selenium sulfide, or zinc pyrithione) if you have flaking/itchiness. A healthy scalp is a foundation for healthy hair.
When to See a Specialist: Your Action Plan
Don't guess. See a professional if:
- You have rapidly increasing visibility.
- You have scaling, itching, pain, or redness on the scalp.
- You're under 25 and seeing significant crown thinning (early-onset pattern loss).
- You're a woman with male-pattern baldness (temples receding, classic bald spot), as this can indicate a hormonal issue.
- You have sudden, patchy hair loss.
Who to see: A board-certified dermatologist with a specialization in hair disorders (trichology) is the gold standard. They can perform a dermatoscope examination (trichoscopy), run blood tests (for iron, thyroid, hormones), and provide an accurate diagnosis. Avoid "hair loss clinics" with high-pressure sales tactics; seek unbiased medical advice.
Conclusion: Your Crown, Your Confidence
So, how much crown visibility is normal? The most honest answer is: the amount that has been stable for you since your early adulthood, adjusted for the slow, inevitable thinning of aging. A few extra strands of scalp showing at 50 may be perfectly normal for your genetic blueprint. The problem arises when that visibility increases noticeably and progressively.
The journey with crown visibility is deeply personal. It’s about separating the natural narrative of aging from the active story of hair loss. By arming yourself with knowledge—understanding the anatomy, recognizing the red flags, identifying potential causes, and exploring the arsenal of solutions—you move from a place of anxiety to one of empowered action. Whether your path leads to medical treatment, cosmetic camouflage, or simply peace of mind with your natural pattern, the first and most crucial step is an honest assessment and, when in doubt, a consultation with a hair specialist. Your crown is more than just the top of your head; it's a part of your identity. Treat it with the informed care it deserves.