How Long Is An Epidural Needle? The Surprising Truth About Size And Safety
Have you ever found yourself lying in a hospital bed, about to undergo a major surgical procedure or preparing for childbirth, and wondered, “How long is an epidural needle?” It’s a question that sparks a mix of curiosity and understandable anxiety. The image of a long, intimidating needle approaching your spine can be daunting. But the reality is far more nuanced and fascinating than the simple number you might imagine. The length of an epidural needle isn't a one-size-fits-all measurement; it's a carefully selected tool in a complex medical procedure, chosen based on a unique combination of patient anatomy, procedural goals, and clinical expertise. Understanding this detail unlocks a deeper appreciation for the precision and safety of modern pain management techniques like epidural analgesia and anesthesia.
This isn't just a trivia question for medical students. For patients, knowing the "why" behind the needle's length can demystify the process, alleviate fears, and empower you to have more informed conversations with your anesthesiologist. For anyone curious about medical procedures, it's a window into the intricate science of accessing the human nervous system. So, let's pull back the curtain and explore the precise measurements, the critical factors that influence the choice, and what that needle actually does once it's in place. The answer might just change how you view one of medicine's most common—and crucial—interventions.
The Short Answer: It's Not About Length, It's About Location
When people ask "how long is an epidural needle," they often picture a single, standard length. The common misconception is that anesthesiologists use a uniformly long needle to reach the spinal canal. In truth, the epidural needle itself is typically between 3 to 5 inches (7.5 to 12.7 centimeters) long. However, this is only part of the story. The critical factor isn't how much of the needle is inserted, but where the tip of that needle needs to go.
The target is the epidural space, a potential space just outside the dura mater, the tough protective membrane surrounding the spinal cord and cerebrospinal fluid. This space is incredibly shallow—often just a few millimeters deep from the skin surface in most adults, though it varies. The needle's primary job is to traverse the layers of tissue (skin, subcutaneous fat, ligaments like the supraspinous and interspinous ligaments, and the ligamentum flavum) to reach this precise location without puncturing the dura. Therefore, the inserted length is usually just 2 to 4 centimeters for most adults. The extra length on the needle provides the anesthesiologist with a secure grip and allows for adjustments during the procedure. So, while the tool is several inches long, only a small fraction of it enters the body.
Key Factors That Determine the "Right" Needle Length and Type
The selection of a specific epidural needle is a clinical decision based on several patient-specific and procedural factors. It’s a tailored approach, not a standard issue.
1. Patient Anatomy: The Primary Determinant
The most significant factor is the patient's own physical build. Anesthesiologists assess:
- Body Mass Index (BMI): For patients with higher BMI and more subcutaneous fat, a longer needle (closer to 5 inches or 12 cm) may be necessary to ensure the tip can reach the ligamentum flavum and identify the epidural space through the "loss of resistance" technique. The extra length compensates for the increased tissue depth.
- Spinal Anatomy: The height of individual vertebrae, the width of the interlaminar spaces (the gaps between the bones of the spine), and the presence of conditions like scoliosis or previous spinal surgery can drastically alter the approach. A shorter needle might be selected for a very thin patient or a child, while a longer, more curved needle might be needed to navigate around bony obstructions.
- Age: Elderly patients often have calcified ligaments and decreased epidural space fat, which can make identification trickier. Needle choice may adapt to these age-related anatomical changes.
2. The Type of Procedure: Epidural vs. Spinal
This is a crucial distinction that often causes confusion.
- Epidural Anesthesia/Analgesia: As discussed, a longer Tuohy needle (the standard for epidurals) is used to place a catheter into the epidural space for continuous medication delivery. The needle is removed after catheter placement.
- Spinal (or "Subarachnoid") Anesthesia: For a single-shot spinal block (common for C-sections), a much shorter, thinner needle (typically 3.5 to 5 cm / 1.5 to 2 inches long) is used. This needle must pierce the dura mater to inject medication directly into the cerebrospinal fluid (CSF) in the subarachnoid space. The target is different, and the needle is designed for a one-time puncture, not catheter placement. This is why a "spinal needle" is often shorter than an "epidural needle," though the initial skin penetration depth can be similar.
3. Needle Design and Gauge (Width)
Length isn't the only specification. Gauge (thickness) is equally important.
- Common Epidural Needle Gauges: Range from 14G (very large, for placing large-bore catheters) to 22G (smaller, for pediatric or sensitive patients). The most common for adult obstetric and surgical epidurals is 16G or 18G.
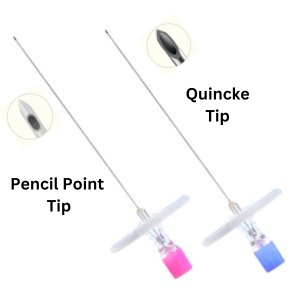
- Needle Tip Design: The Tuohy needle has a curved, blunt-tipped end. This design is intentional—it is blunt to reduce the risk of puncturing the dura and blood vessels, and curved to help deflect the dura away from the needle tip as it enters the epidural space. The curve also aids in directing the catheter correctly. In contrast, spinal needles (like the Quincke or Whitacre) have a sharp, pencil-point tip designed to make a clean, small puncture in the dura with minimal CSF leakage and post-procedure headache.
A Detailed Look at the Epidural Procedure: From Skin to Space
Understanding the journey of the needle clarifies why its specifications matter. Here is a step-by-step breakdown of a standard lumbar epidural placement.
Step 1: Preparation and Positioning
The patient is usually seated, leaning over a table, or lying on their side in the fetal position. This position maximizes the interlaminar spaces between the vertebrae, creating the widest possible "window" to the epidural space. The anesthesiologist identifies the correct vertebral level (typically L3-L4 or L4-L5 for adults, well below the end of the spinal cord at L1-L2) by palpating the iliac crests (the top of the hip bones), which align roughly with L4.
Step 2: Skin Anesthesia and Initial Insertion
The skin and deeper tissues are numbed with a small amount of local anesthetic (like lidocaine) using a very fine, short needle (27G or 25G). This step minimizes the discomfort of the larger epidural needle's entry. The epidural needle, attached to a syringe containing either air or saline, is then introduced perpendicular to the skin (or with a slight cephalad angle) and advanced slowly.
Step 3: Navigating the Ligaments – The "Loss of Resistance" Technique
This is the critical moment. The anesthesiologist advances the needle in small increments, feeling for a distinct change in resistance.
- As the needle passes through the supraspinous and interspinous ligaments, there is a gritty, fibrous resistance.
- It then penetrates the ligamentum flavum, a strong, elastic ligament. Here, the resistance becomes firm and taut.
- The "loss of resistance" occurs the moment the needle tip breaches the ligamentum flavum and enters the epidural space. The anesthesiologist feels a sudden "give" or drop in pressure. At this exact instant, they stop advancing. For a "loss of resistance to air" technique, a small puff of air is injected to confirm the space (no resistance means it's not in tissue or blood vessel). For "loss of resistance to saline," a drop of saline is observed to flow freely into the syringe.
Step 4: Catheter Placement and Needle Removal
Once the epidural space is confirmed, a flexible plastic catheter is threaded through the needle's lumen into the space, typically 3-5 cm deep. The needle is then carefully withdrawn, leaving the catheter in place. The catheter is secured to the skin with tape and connected to a filter and infusion pump or a manual syringe for delivering local anesthetics (like bupivacaine) and/or opioids (like fentanyl).
Step 5: Testing the Block
A small test dose of medication is administered through the catheter to ensure it is not intravascular (in a blood vessel) or intrathecal (in the CSF). The anesthesiologist monitors for signs of systemic toxicity or a rapid, high spinal block. Once safety is confirmed, the full dose is given, and the desired sensory and motor block develops over 10-20 minutes.
Risks, Complications, and the Role of Needle Choice
While epidurals are extremely safe when performed by trained professionals, no procedure is without risk. The design and size of the needle are directly linked to minimizing these risks.
- Post-Dural Puncture Headache (PDPH): This is the most common complication related to needle size. If the Tuohy needle accidentally punctures the dura mater, CSF can leak, causing a severe headache when upright. The larger the needle gauge (smaller number), the higher the risk of PDPH. This is why some anesthesiologists may opt for a smaller gauge (e.g., 18G vs. 16G) in patients at higher risk, such as young women. The blunt tip of the Tuohy is also designed to push the dura aside rather than cut it, reducing risk compared to a sharp spinal needle.
- Epidural Hematoma: Bleeding into the epidural space, which can compress the spinal cord. Risk is increased with anticoagulant use, bleeding disorders, or difficult, multiple attempts. Using the smallest effective gauge and a single, smooth pass reduces trauma.
- Nerve Injury: Direct trauma from the needle tip is rare with proper technique but is a severe risk. The curved, blunt Tuohy tip is designed to be "nerve-sparing," pushing nerves aside rather than piercing them. Multiple attempts or patient movement during insertion increase this risk.
- Infection: Strict sterile technique is paramount. The needle's length and design do not directly influence infection risk, which is more related to aseptic protocol and catheter management.
- Inadequate or Failed Block: This can occur if the catheter is not in the optimal position. Needle length and angle of insertion influence catheter path. A needle that is too short for the patient's anatomy may not allow the catheter to be threaded far enough into the space to be effective.
Frequently Asked Questions About Epidural Needles
Q: Does a longer needle mean more pain?
A: Not necessarily. The discomfort is most intense at the skin and as the needle penetrates the ligamentum flavum. The length of the needle shaft outside your body doesn't correlate with pain. A skilled anesthesiologist uses local anesthetic at each layer and advances the needle slowly. The gauge (thickness) has a more significant impact on discomfort than the overall length.
Q: Can I request a specific needle size?
A: You can certainly discuss your concerns with your anesthesiologist. They will choose the needle based on your anatomy, medical history, and the planned procedure. For example, if you are a young, thin female with a history of severe migraine headaches (a risk factor for PDPH), you might discuss the option of a smaller gauge needle (e.g., 18G instead of 16G). However, the final decision rests with the clinical expert to ensure safety and efficacy.
Q: How far does the needle actually go in?
A: For the vast majority of adults, the distance from the skin to the epidural space at the lumbar level is between 2 and 4 centimeters (about 0.8 to 1.6 inches). The anesthesiologist knows they've reached the space by the "loss of resistance" feel. The rest of the needle's length remains outside your back, providing a handle for control.
Q: Is the epidural needle the same as the one used for a spinal block?
A: No. While both access the spine, they are different tools for different jobs. An epidural needle (Tuohy) is longer, has a curved blunt tip, and is used to place a catheter. A spinal needle is shorter, has a very fine, sharp pencil-point tip (like a Whitacre or Sprotte), and is used for a single injection directly into the CSF. Sometimes, a "combined spinal-epidural" (CSE) is performed, where a special needle is used to first give a spinal dose and then place an epidural catheter through the same needle or a separate one.
Q: What happens if the first attempt fails?
A: It's not uncommon to require more than one attempt, especially in patients with challenging anatomy. The anesthesiologist will withdraw the needle, re-assess the position, and try again, possibly at a different interspace (e.g., moving from L4-L5 to L3-L4). Each attempt uses a new, sterile needle. Communication is key—let your provider know if you're feeling significant pain or discomfort during adjustments.
Conclusion: Precision Over Panic
So, how long is an epidural needle? The tool in the anesthesiologist's tray is typically 3 to 5 inches long, but the part that enters your back is usually only about 1 to 1.5 inches. This seemingly small detail is the product of decades of medical innovation, designed with one paramount goal: to deliver life-changing pain relief with the absolute minimum risk. The length, gauge, and tip design are not arbitrary; they are a calculated response to the complex, variable landscape of human anatomy.
The next time you hear the term "epidural needle," remember it's not a symbol of fear, but a testament to precision medicine. It represents a careful negotiation with the body's own architecture, guided by a clinician's skilled hands and deep understanding. The real measure of its success isn't in centimeters, but in the relief it provides—the mother who can breathe through labor, the patient who can undergo major surgery without the trauma of general anesthesia, the individual who finds comfort in their most vulnerable moments. That is the true, powerful length of the epidural needle: the distance between profound pain and profound peace.