Why Do The English Have Bad Teeth? Debunking A Persistent Stereotype
Why do the English have bad teeth? This question, often posed with a mix of curiosity and casual prejudice, has become a pervasive cultural cliché. From American sitcoms to casual international banter, the image of imperfect British smiles is a trope as familiar as tea and rainy weather. But is this stereotype rooted in reality, or is it an outdated myth? The truth is far more complex and interesting than the joke suggests. It involves a fascinating mix of historical public health policy, cultural attitudes, socioeconomic factors, and even a dash of Hollywood exaggeration. This article will thoroughly dissect the origins, realities, and modern evolution of dental health across England, moving beyond the simplistic gag to understand the full picture.
The Historical Roots: Where the Stereotype Began
To understand the present, we must first look to the past. The "bad teeth" stereotype didn't emerge in a vacuum. It has concrete historical foundations that explain why the perception took hold, even if it no longer fully reflects current realities.
Post-War Britain and the Lack of Universal Dental Care
Following World War II, the UK established the National Health Service (NHS) in 1948, a revolutionary concept providing healthcare free at the point of use. However, dental care was treated differently. While the NHS initially offered free dental treatment, this was drastically scaled back by the 1950s. Charges were introduced for dentures (1951) and then for other treatments (1952), leading to the famous "false teeth" sign protests. This created a system where dental care was often seen as a private, optional expense rather than an integral part of universal healthcare. For decades, regular dental check-ups were not a cultural norm for the working class, leading to preventable decay and extractions becoming common. The NHS model focused on treatment, not prevention, for many years.
The Cultural Attitude: Teeth as Functional, Not Cosmetic
In many cultures, particularly the United States, a bright, straight, white smile is a major social asset and status symbol. In contrast, traditional British culture has historically viewed teeth more pragmatically: as tools for eating. The emphasis was on function over form. A tooth that could chew was a good tooth, regardless of its colour or alignment. This cultural mindset meant that cosmetic dentistry—veneers, whitening, extensive orthodontics—was, and for many still is, seen as an unnecessary vanity rather than a standard part of self-care. This fundamental difference in values is a core reason for the visual discrepancy that fueled the stereotype.
The Sugar Tax and Dietary Shifts
The UK's relationship with sugar has played a significant role. While sugar consumption is high globally, historically, sugary tea, biscuits, and sweets were—and remain—deeply ingrained in British daily life and social rituals. The widespread availability of cheap, sugary foods and drinks, particularly in the post-war period, contributed to poor dental health, especially in children. It's only in recent decades that public health campaigns and, more recently, the Sugar Tax (Soft Drinks Industry Levy) introduced in 2018, have begun to actively combat this.
The Modern Reality: Is the Stereotype Still True?
This is the most critical question. The short answer is: the stereotype is increasingly outdated, but its shadow lingers due to persistent inequalities.
The Data: How Does the UK Actually Compare?
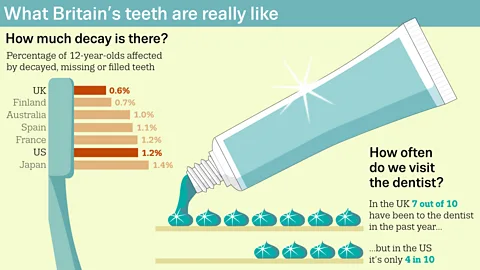
Let's look at the hard numbers. According to the World Health Organization (WHO), the UK has seen massive improvements in dental health over the last 30 years. The average number of decayed, missing, or filled teeth (DMFT) for 12-year-olds has plummeted. However, comparisons with other developed nations tell a nuanced story.
- A 2015 study by the British Dental Journal comparing OECD countries found that while the UK's dental health for children had improved, it still lagged behind countries like Germany, Sweden, and Switzerland.
- Health inequalities are the defining feature of UK dental health today. A child's oral health is strongly correlated with their parents' socioeconomic status and geographic location. Children in the most deprived areas of England have, on average, over five times more tooth decay than those in the least deprived areas.
- The NHS reports that while 84% of adults in England have at least one filling, and the average adult has around 7 fillings, this masks huge regional and class-based variations.
The Two-Tier System: NHS vs. Private Dentistry
The UK's dental landscape is a hybrid system that contributes to the disparity.
- NHS Dentistry: Provides essential, affordable care (with patient charges). However, it is often over-subscribed, with many practices having long waiting lists and not accepting new NHS patients. The NHS treatment band system (Band 1, 2, 3) can make complex treatments expensive upfront, and the focus remains on necessary treatment rather than cosmetic perfection.
- Private Dentistry: Offers shorter wait times, more advanced cosmetic options (like Invisalign and high-quality veneers), and a more luxurious experience. It is, of course, paid for entirely by the patient. This creates a visible socioeconomic divide in smiles. The perfectly aligned, white teeth of the affluent are increasingly common in London and the Southeast, while in less wealthy areas, the "traditional" look of fillings, crowns, and some missing teeth remains more prevalent. This visible gap is what many international observers pick up on and mistake for a national characteristic.
The Rise of Cosmetic Dentistry and "Hollywood Smiles"
The last 20 years have seen a cosmetic dentistry boom in England. fueled by social media, celebrity culture, and a growing private sector. Procedures like teeth whitening (now widely available), clear aligners (e.g., Invisalign), and porcelain veneers are no longer just for the mega-wealthy. They are mainstream aspirations for the middle class. This means the younger, wealthier generation of English people are now just as likely to have "perfect" smiles as their peers in the US or Australia. The stereotype is aging rapidly.
Key Factors Contributing to Persistent Dental Health Challenges
Even with improvements, several interconnected factors continue to challenge optimal dental health for a significant portion of the English population.
1. Socioeconomic Deprivation and Geographic Inequality
This is the single biggest factor. Poverty and deprivation correlate strongly with poor diet (high in sugar, low in fresh produce), limited access to NHS dentists (due to practice closures in low-income areas or inability to afford patient charges), and lower health literacy. "Dental deserts"—areas with very few NHS dental practices—are a real and growing problem, particularly in the North of England, rural areas, and coastal towns. A child growing up in such an area, without regular access to a dentist and with a diet high in cheap, sugary foods, is at a severe disadvantage from the start.
2. The "Extraction Culture" and Fear of the Dentist
Historically, extraction was the default treatment for problematic teeth. This legacy persists. Some older generations, and even some younger people in deprived areas, still hold the attitude that "just take it out" is a simpler solution than a complex, expensive root canal or crown. This is compounded by dental anxiety—a fear often passed down through families who experienced the more painful, less sophisticated dentistry of the past. The NHS system, while excellent for emergency care, can sometimes feel impersonal and rushed, not always having the time to alleviate deep-seated fears or discuss long-term preventative plans.
3. Dietary Habits and Sugar Consumption
The British love affair with sugar remains a major public health issue. Fizzy drinks, fruit juices (high in natural sugars), sweets, and sugary cereals are consumed in large quantities. The constant snacking and sipping of sugary drinks throughout the day is particularly damaging, as it keeps the mouth's pH acidic, eroding enamel. While awareness is growing, changing deeply ingrained dietary habits is a slow process.
4. The Impact of Smoking and Excessive Alcohol
Smoking is a primary cause of staining, gum disease, and oral cancer. Rates of smoking, while declining, are still higher in deprived communities. Excessive alcohol consumption, also linked to socioeconomic status, contributes to dry mouth (reducing protective saliva) and increases the risk of mouth cancer. These lifestyle factors compound the problems caused by diet and access to care.
5. Orthodontic Access and Timing
The NHS provides free orthodontic treatment (braces) for children with a clear clinical need (using the IOTN scale). However, due to funding constraints and long waiting lists, many children who would benefit from treatment are not referred, or face years of waiting. This means that for many, misaligned teeth—which can be harder to clean and more prone to decay and gum disease—are left untreated until adulthood, when private treatment is the only (and costly) option. This contributes to the higher prevalence of crooked teeth in the general population compared to countries with more generous public orthodontic schemes.
Addressing Common Questions and Related Concerns
Q: Is the "bad teeth" stereotype just American propaganda?
It's not just propaganda, but it is a massive oversimplification. American media, particularly sitcoms like The Simpsons (with its recurring "British dentist" joke) and movies, has certainly amplified and caricatured a kernel of historical truth. They take a real, complex issue of health inequality and reduce it to a lazy national characteristic. The joke is funnier if you believe it's universally true, which it isn't.
Q: Do Brits actually care about their teeth less?
No. The desire for a healthy, attractive smile is universal. What differs is access, priority, and cultural framing. For a family struggling with the cost of living, paying for private dental treatment or even regular NHS check-ups may be a lower financial priority than heating or food. The cultural de-emphasis on cosmetic perfection means they may not feel the same social pressure to spend on whitening or veneers, but the desire for pain-free, functional teeth is absolutely there.
Q: How does England's dental health compare to Scotland, Wales, and Northern Ireland?
The devolved nations have their own NHS systems. Scotland has its own Childsmile programme, a highly regarded preventative initiative for children, which has shown excellent results. Wales has similar targeted programmes. Generally, the patterns of inequality are similar across the UK, with health outcomes closely tied to deprivation. The stereotype is usually directed specifically at "the English," but the underlying systemic issues are UK-wide.
Q: What can individuals do to improve their dental health?
Regardless of the system, personal agency is powerful:
- Brushing & Flossing: Brush twice daily with fluoride toothpaste for two minutes. Use floss or interdental brushes daily. This is non-negotiable.
- Dietary Awareness: Drastically reduce frequency of sugary snacks and drinks. Choose water or milk. Consume sugar primarily with meals.
- Regular Check-ups: See a dentist as often as they recommend, even if you have no pain. Prevention is cheaper and less distressing.
- Fluoride: Use a fluoride mouthwash if recommended by your dentist. Fluoride varnish applications are a great preventative measure.
- Advocacy: If you live in a "dental desert," lobby your local MP and Clinical Commissioning Group (CCG) for better provision. Community pressure can drive change.
The Path Forward: NHS Reform and Changing Perceptions
The future of English dental health hinges on two parallel tracks: systemic reform and cultural shift.
Reinventing NHS Dentistry for Prevention
There is growing political and professional consensus that the NHS dental contract, which largely pays dentists per treatment ( incentivizing quantity over quality), needs radical reform. The ideal is a system that rewards preventative care, manages populations' oral health proactively, and ensures equitable access. Initiatives like expanding water fluoridation (currently only covering about 10% of the population) are evidence-based public health measures that could dramatically reduce decay, especially in deprived areas.
Eroding the Stigma and Embracing Prevention
Culturally, the message is slowly changing. Public Health England's campaigns, the Sugar Tax, and greater media focus on health inequalities are helping. The goal is to make regular dental check-ups as normal and unremarkable as visiting the GP, and to shift the national conversation from "fixing bad teeth" to "maintaining good teeth for life." The growing popularity of private cosmetic dentistry also signals that the desire for an attractive smile is strong—the challenge is making good oral health and basic cosmetic outcomes accessible to all, not just the wealthy.
Conclusion: Beyond the Stereotype
So, why do the English have bad teeth? The flippant answer is a lazy cultural stereotype. The real answer is a story of historical under-investment in public dental prevention, a healthcare system that has struggled with access and equity, and socioeconomic inequalities that manifest plainly in the mouth. It is a story of a cultural attitude that long prioritized function over aesthetics, now clashing with a globalized, image-conscious world.
The good news is that the narrative is changing. Dental health in England has improved dramatically and continues to do so for many. The "bad teeth" image is becoming a caricature of a bygone era, increasingly at odds with the reality of a population where cosmetic dentistry is booming and where, for those with means, excellent dental care is readily available. The true challenge—and the real story—is not about the English as a monolithic group, but about tackling the deep-rooted health disparities that mean a person's postcode, more than their nationality, remains the strongest predictor of their oral health. The goal is no longer to defend against a stereotype, but to ensure that a healthy smile is a possibility for everyone, regardless of where they live or how much they earn.