Where Does The Egg Go After Tubal Ligation? The Surprising Science Explained
Have you ever wondered, where does the egg go after tubal ligation? It’s one of the most common and logical questions women have when considering this permanent form of birth control. The procedure is often described as "tying the tubes," but what actually happens to the monthly egg that is no longer able to travel to the uterus? The answer is a fascinating journey into female anatomy and physiology, and it’s not what most people assume. Understanding this process is crucial for making an informed decision about your reproductive health and dispelling common myths.
Tubal ligation, commonly known as "getting your tubes tied," is a surgical procedure performed on over 600,000 women in the United States annually. It is a highly effective, permanent contraceptive method. Yet, a cloud of confusion often surrounds the fate of the ovum, or egg, after the fallopian tubes are blocked. This article will demystify the entire process, from the moment of ovulation to the final absorption of the egg, providing a clear, science-based explanation. We will explore the biological mechanisms, address concerns about hormonal changes, discuss the rare phenomenon of ectopic pregnancy, and examine alternatives. By the end, you will have a comprehensive understanding of your body’s remarkable ability to handle this change seamlessly.
The Mechanics of Tubal Ligation: A Blocked Pathway
What Exactly is Tubal Ligation?
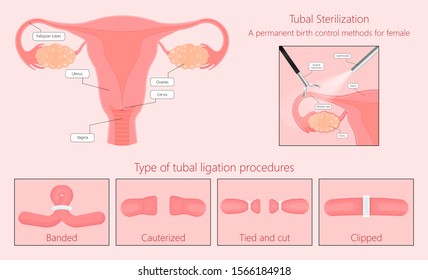
Tubal ligation is a surgical procedure designed to create a permanent blockage in the fallopian tubes. The fallopian tubes are two thin, trumpet-shaped structures that extend from the uterus toward the ovaries. Their primary function is to capture the egg released during ovulation and provide the site for fertilization with sperm. The fertilized egg, now a zygote, then travels down the tube to implant in the uterine lining. During tubal ligation, a surgeon uses one of several methods—clips, rings, electrocautery (burning), or complete removal of a segment—to obstruct this pathway. The most common modern techniques include the Filshie clip or Hulka clip, which clamp the tube, and bipolar coagulation, which seals it with heat.
The procedure is typically performed laparoscopically, a minimally invasive surgery involving small incisions in the abdomen. Sometimes, it is done postpartum (after a vaginal delivery or C-section) or during a cesarean section. Regardless of the timing or method, the goal is singular: to prevent the egg and sperm from meeting by creating an insurmountable physical barrier. The ovaries themselves remain completely untouched and fully functional, continuing their hormonal symphony and releasing eggs as usual.
The Critical Distinction: Ovaries vs. Fallopian Tubes
A fundamental point of confusion must be clarified immediately. Tubal ligation does not affect the ovaries. The ovaries are the reproductive organs responsible for producing eggs (ova) and secreting the hormones estrogen and progesterone. The fallopian tubes are merely the transport system. Therefore, after tubal ligation:
- Ovulation continues: The ovary still releases a mature egg during each menstrual cycle.
- Hormone production is unchanged: The menstrual cycle, including hormonal fluctuations, remains virtually identical to pre-procedure cycles. There is no induced menopause or early decline in estrogen.
- Uterine lining still builds up: Under the influence of hormones, the endometrium (uterine lining) thickens in preparation for a potential pregnancy.
This distinction is the key to understanding the egg’s fate. The egg is released into the abdominal cavity, near the fimbriae (the finger-like ends of the fallopian tubes), but the tube is now blocked, so it cannot enter.
The Journey’s End: Where Does the Egg Actually Go?
Absorption Within the Abdominal Cavity (Peritoneal Cavity)
So, if the egg is released but cannot enter the fallopian tube, where does it go? The answer is simple and elegant: it is harmlessly absorbed by the body. When the ovary releases an egg during ovulation, it is not shot directly into a tube. Instead, the egg is expelled from the ovarian follicle into the peritoneal cavity—the fluid-filled space within the abdomen that houses the intestines, liver, and other organs. The fimbriae of the fallopian tube normally sweep over the ovary to catch the egg and guide it inside.
After a successful tubal ligation, this pathway is obstructed. The egg, now a single cell, simply floats in the peritoneal fluid. Within hours to a couple of days, it undergoes a natural process of degeneration and is phagocytosed—engulfed and digested—by specialized immune cells called macrophages. These cells are part of the body’s constant cleanup crew, removing dead cells, debris, and foreign material from the abdominal cavity. The resulting nutrients and cellular components are recycled by the body. This process is identical to how the body handles any other cell that dies and needs to be removed. There is no "backup," no accumulation, and no harm. It is a silent, efficient, and completely normal physiological event that occurs with every cycle post-ligation.
Debunking the Myth: The Egg Does Not Cause Cysts or Pain
A persistent myth suggests that the unreleased egg causes ovarian cysts or chronic pelvic pain. This is not supported by medical science. While some women may experience post-ligation pain syndrome (a separate condition often related to surgical trauma or nerve irritation), it is not caused by the presence of an unabsorbed egg. Ovarian cysts are fluid-filled sacs that develop on the ovary itself, related to the egg’s development process (like follicular cysts) or other hormonal factors, not to the egg’s final destination after release. The monthly release and subsequent absorption of the egg is a non-event from a symptomatic perspective for the vast majority of women.
Hormonal Harmony: Why Your Period Stays the Same
The Ovarian Hormone Pipeline Remains Intact
A major concern for many is whether tubal ligation will trigger early menopause or cause drastic hormonal swings. The resounding answer is no. Because the ovaries are left intact and their blood supply is preserved, they continue to produce estrogen and progesterone in a normal, cyclical pattern. The hormonal feedback loop involving the hypothalamus and pituitary gland in the brain remains completely undisturbed.
You will continue to have a monthly menstrual cycle, albeit one that is not resulting in pregnancy. Your periods may even become slightly more regular, as the stress of potential pregnancy is removed from the system. Any changes in menstrual flow or symptoms are usually coincidental or related to age, not the ligation itself. If you experience significant changes like heavy bleeding or severe pain after the procedure, it is important to consult your doctor to rule out other causes, such as endometriosis or fibroids, which are unrelated to the tubal blockage.
The Role of Progesterone and the Luteal Phase
After ovulation, the ruptured follicle transforms into the corpus luteum, a temporary endocrine structure that secretes progesterone. Progesterone is essential for preparing the uterine lining for implantation. In a non-pregnancy cycle, the corpus luteum degenerates after about 14 days, progesterone levels drop, and the uterine lining sheds—this is menstruation. This entire hormonal sequence continues unchanged after tubal ligation. The egg may not be fertilized, but the corpus luteum still forms and produces progesterone for its typical lifespan. The body does not "know" the egg wasn't fertilized until the usual time, so the hormonal ebb and flow proceed as clockwork.
The Rare Exception: Understanding Ectopic Pregnancy Risk
What is an Ectopic Pregnancy and How Does It Relate?
While tubal ligation is over 99% effective at preventing pregnancy, there is a very small chance of failure. The most serious type of failure is an ectopic pregnancy, where a fertilized egg implants outside the uterus, most commonly in a fallopian tube. This is a life-threatening medical emergency. After tubal ligation, if pregnancy does occur (about 1 in 200 women), there is a higher proportion of these being ectopic.
Why does this happen? It is usually due to fistula formation. In rare cases, the blocked ends of the fallopian tube can spontaneously create a tiny, new opening (a fistula) that allows sperm to pass through but is too narrow for the fertilized egg to travel back to the uterus. The fertilized egg then implants in the tube itself, which cannot stretch to accommodate a growing pregnancy and can rupture. This is why any woman with a history of tubal ligation who experiences a missed period, pelvic pain, or abnormal vaginal bleeding must seek immediate medical attention to rule out ectopic pregnancy. It is a critical safety point.
Symptoms of a Post-Ligation Ectopic Pregnancy
Early recognition is vital. Symptoms can include:
- Sharp, stabbing pain in the pelvis, abdomen, or shoulder.
- Vaginal spotting or bleeding.
- Dizziness, fainting, or signs of shock (pale skin, rapid pulse).
- Rectal pressure.
These symptoms typically appear between 6 and 10 weeks of pregnancy. If you have had a tubal ligation and suspect you might be pregnant, an urgent pregnancy test and ultrasound are mandatory.
Reversibility and Alternatives: Planning for the Future
Is Tubal Ligation Reversible? The Reality of Tubal Reanastomosis
Tubal ligation is considered a permanent contraceptive method. However, a surgical procedure called tubal reversal (tubal reanastomosis) exists. This is a complex, delicate microsurgery where the blocked segments of the fallopian tube are removed and the two healthy ends are meticulously sutured back together. Success rates vary dramatically based on:
- The original ligation method (clips and rings have higher reversal success than electrocautery).
- The age of the woman (younger women have higher success rates).
- The length of remaining healthy tube.
- The surgeon's skill.
Pregnancy rates after a successful reversal range from 40% to 70%, but the risk of ectopic pregnancy remains elevated. It is a major surgery with no guarantees, often costing thousands of dollars, and is not typically covered by insurance for contraceptive reversal. Therefore, tubal ligation should only be chosen by women who are absolutely certain they do not want future biological children.
Long-Acting Reversible Contraceptives (LARCs) as Alternatives
For women seeking highly effective, long-term birth control but who want to retain the option of future pregnancy, Long-Acting Reversible Contraceptives (LARCs) are excellent alternatives. These include:
- Hormonal IUDs (e.g., Mirena, Kyleena): Inserted into the uterus, release progestin, last 3-8 years. Highly effective, can make periods lighter or stop them.
- Copper IUD (Paragard): Non-hormonal, uses copper to prevent sperm from fertilizing the egg. Can last up to 10-12 years. May cause heavier periods initially.
- Contraceptive Implant (Nexplanon): A small rod inserted in the upper arm, releases progestin, effective for up to 5 years.
These methods are over 99% effective, comparable to tubal ligation, but are completely reversible. Fertility returns quickly after removal. They offer flexibility without surgery.
Addressing Common Questions and Concerns
Will I Still Have a Period? What About Menopause?
Yes, you will still have periods. As explained, your hormonal cycle continues. You will experience monthly menstrual bleeding as the uterine lining sheds. The timing, flow, and symptoms should remain largely the same, though some women report lighter periods post-ligation. You will not go through early menopause. Menopause is determined by ovarian reserve and function, which tubal ligation does not affect. You will enter natural menopause at the same age you would have without the procedure.
Can I Get Pregnant After Tubal Ligation?
There is a small, but real, risk of post-sterilization pregnancy. The failure rate is approximately 1 in 200 (0.5%). This can happen if the tubes spontaneously re-canalize (form a new connection), if a fistula develops, or if the surgery was not completed correctly initially. This is why some doctors recommend a follow-up hysterosalpingogram (HSG) X-ray to confirm tubal blockage, though it's not routine. If you miss a period after tubal ligation, take a pregnancy test immediately.
What About the Egg and Hormones if I Have My Tubes Removed (Salpingectomy)?
An increasingly common variation is a complete bilateral salpingectomy, where the entire fallopian tubes are removed. This is sometimes done for cancer risk reduction (as some ovarian cancers originate in the tubes) or as a more definitive sterilization. The fate of the egg is identical. The ovary still releases the egg into the peritoneal cavity, where it is absorbed. The hormonal function is 100% preserved because the ovaries are untouched. This procedure eliminates the rare risk of tubal ectopic pregnancy entirely, as there is no tube for an embryo to implant in.
Making the Decision: Is Tubal Ligation Right for You?
Key Considerations Before Proceeding
Choosing permanent contraception is a significant decision. Key factors to contemplate include:
- Certainty: Are you absolutely sure you do not want any (or any more) biological children? Consider your partner's wishes, your life goals, and your age.
- Alternatives: Have you fully explored LARCs or your partner's options like a vasectomy (which is simpler, cheaper, and also highly effective)?
- Health: Are there any personal or family medical history factors that might influence your choice?
- Surgical Risks: Like any surgery, there are risks of infection, bleeding, or damage to surrounding organs (though very low with laparoscopy).
- Regret: Studies show regret is higher in younger women (under 30) and those who have not yet had children. Be honest with yourself.
The Importance of Informed Consent
A reputable healthcare provider will engage in a thorough informed consent process. They will discuss:
- The permanent nature of the procedure.
- All alternatives, including their effectiveness and reversibility.
- The specific method they plan to use and why.
- The surgical procedure, anesthesia, and recovery.
- The small risk of failure and ectopic pregnancy.
- The fact that it does not protect against STIs.
- That your periods and hormones will continue.
Do not hesitate to ask questions. Request pamphlets or trusted online resources (like those from the American College of Obstetricians and Gynecologists - ACOG). This is your body and your future.
Conclusion: A Silent, Efficient Process
So, to directly answer the question where does the egg go after tubal ligation: it is released by the ovary into the abdominal cavity and is quietly, efficiently absorbed by the body’s immune system within days. Your hormonal cycle continues uninterrupted, your periods persist, and your body functions exactly as it did before, minus the possibility of pregnancy. The process is a testament to the body’s elegant waste management system.
Tubal ligation is a powerful, permanent tool for family planning. Its effectiveness hinges on a simple physical principle: blocking the passage. The egg’s journey ends not in a mysterious place, but in the same cellular recycling bin that handles millions of dead cells in your body every day. Understanding this science empowers you to make a confident, informed choice about your reproductive health, free from myths and misconceptions. If you have lingering questions after reading this, the best next step is a detailed conversation with your gynecologist, who can provide personalized guidance based on your unique health profile and life circumstances.