Blue Bloater Vs Pink Puffer: Decoding COPD's Classic Faces
Have you ever heard the terms "blue bloater" and "pink puffer" and wondered what they really mean? These vivid nicknames describe two classic, yet contrasting, presentations of Chronic Obstructive Pulmonary Disease (COPD), a progressive lung condition that makes it hard to breathe. While modern medicine recognizes that most patients exhibit a mix of both traits, understanding these archetypes remains crucial for grasping COPD's complexity, its underlying mechanisms, and why personalized treatment is so vital. This article will dive deep into the blue bloater vs pink puffer comparison, exploring their characteristics, the science behind them, and what it means for millions living with this disease.
Understanding the Foundations: COPD and Its Two Main Components
Before dissecting the phenotypes, we must understand the disease they represent. COPD is not a single disease but an umbrella term for progressive lung diseases that obstruct airflow. The two primary conditions under this umbrella are chronic bronchitis and emphysema. The classic "blue bloater" is primarily associated with chronic bronchitis, while the "pink puffer" is emblematic of emphysema. However, it's increasingly common for individuals to have features of both, a condition often termed "mixed COPD." The Global Initiative for Chronic Obstructive Lung Disease (GOLD) reports that COPD is the third leading cause of death worldwide, highlighting the critical need for public awareness and understanding of its manifestations.
What is Chronic Bronchitis? The "Blue Bloater" Foundation
Chronic bronchitis is clinically defined by a productive cough that lasts for at least three months, occurring in at least two consecutive years. Its core problem is inflammation and thickening of the bronchial tubes, accompanied by excessive mucus (sputum) production. This mucus plugs the airways, causing a persistent cough as the body tries to clear it. The chronic inflammation also leads to scarring and narrowing of the airways, creating significant airflow obstruction. This obstruction is often more pronounced during exhalation, trapping air in the lungs.
What is Emphysema? The "Pink Puffer" Foundation
Emphysema, on the other hand, involves the gradual destruction of the alveoli—the millions of tiny, delicate air sacs at the end of the bronchioles where oxygen and carbon dioxide exchange occurs. Think of a healthy lung as a fresh, springy sponge full of tiny bubbles (alveoli). In emphysema, the walls between these bubbles break down, creating larger, fewer, and floppy air spaces. This reduces the total surface area for gas exchange and diminishes the lung's elastic recoil. The lungs lose their natural "push" to expel air, leading to air trapping and hyperinflation—the lungs become permanently over-inflated, like an overstretched balloon.
The Classic "Pink Puffer": The Emphysema-Dominant Profile
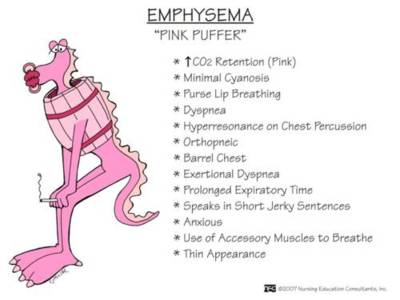
The "pink puffer" nickname paints a clear picture: someone who is often thin, appears to be "puffing" or pursing their lips to breathe, and maintains a relatively normal skin color ("pink"). This presentation is more commonly associated with centriacinar emphysema, which typically affects the upper lobes of the lungs first and is strongly linked to a history of smoking.
Physical Appearance and Body Composition
A classic pink puffer is frequently underweight or has a low body mass index (BMI). This wasting, sometimes called "pulmonary cachexia," occurs because the immense work of breathing burns a tremendous number of calories. The diaphragm, which should be dome-shaped, becomes flattened and inefficient due to hyperinflation. Accessory muscles in the neck and shoulders (like the sternocleidomastoid) work overtime to help lift the rib cage and draw air in. This constant muscular exertion contributes to the lean, sometimes even wasted, appearance. They may also develop barrel chest—a rounded, expanded chest—from the chronically hyperinflated lungs.
Breathing Pattern and Symptoms
The hallmark is rapid, shallow breathing with noticeable pursed-lip breathing (PLB). Pursed-lip breathing is a clever, subconscious adaptation: by exhaling against pursed lips, the patient creates back-pressure in the airways, keeping them open longer and allowing more trapped air to escape. This helps improve gas exchange and reduces the feeling of breathlessness (dyspnea). They often experience minimal cough and sputum production early on because their primary issue is alveolar destruction, not significant mucus hypersecretion. Their main complaint is progressive dyspnea on exertion, which can eventually occur even at rest. They may describe a constant feeling of "air hunger."
Blood Gases and Oxygenation
The term "pink" refers to relatively normal blood oxygen levels (PaO2) and low carbon dioxide levels (PaCO2) in the earlier stages. Why? Their hyperventilation—breathing fast and deep—effectively blows off carbon dioxide. However, as emphysema progresses and the lung surface area vanishes, oxygen levels eventually drop, and carbon dioxide can begin to rise, leading to a bluish tinge (cyanosis) later in the disease.
The Classic "Blue Bloater": The Chronic Bronchitis-Dominant Profile
The "blue bloater" conjures an image of someone who is overweight or swollen ("bloated"), has a chronic cough producing lots of mucus, and exhibits a bluish discoloration of the skin and mucous membranes ("blue") due to low oxygen. This phenotype is linked to chronic bronchitis and often presents with chronic hypoxemia and hypercapnia (high CO2) earlier in the disease course.
Physical Appearance and Body Composition
Blue bloaters are often overweight or have a normal to increased BMI. The "bloater" aspect can come from two sources: obesity itself and peripheral edema (swelling in the ankles and legs). This edema is a sign of right-sided heart failure, known as cor pulmonale. The chronic low oxygen levels (hypoxemia) cause the pulmonary arteries to constrict and stiffen, increasing pressure in the right ventricle of the heart, which eventually fails. They may also have cyanosis, a bluish tint, most visible on the lips, fingertips, and nail beds, due to deoxygenated hemoglobin in the blood.
Breathing Pattern and Symptoms
Their breathing is often slower and more labored compared to the pink puffer's rapid breaths. They typically have a productive cough with frequent sputum production, especially in the mornings. This cough is a direct result of the inflamed, mucus-hypersecreting airways. While they experience dyspnea, it may be less dramatic at rest than in a severely hyperinflated pink puffer, but it is compounded by the weight they carry and the inefficiency of their oxygen exchange. They are more prone to frequent respiratory infections (exacerbations) because the stagnant mucus is a perfect breeding ground for bacteria.
Blood Gases and Oxygenation
The "blue" is clinically significant. Blue bloaters commonly have chronically low arterial oxygen (PaO2) and elevated carbon dioxide (PaCO2) levels, even at rest. This is because their primary problem is ventilation-perfusion mismatch: some lung areas are poorly ventilated due to mucus plugs but still perfused with blood, leading to shunting of deoxygenated blood into the systemic circulation. Their bodies may partially adapt by increasing red blood cell production (polycythemia) to carry more oxygen, but this thickens the blood and strains the heart.
The Underlying Mechanisms: Why Do These Differences Occur?
The divergent phenotypes stem from the different pathological processes at play. In emphysema (pink puffer), the destruction is in the lung parenchyma (the functional tissue). The airways themselves may be relatively intact until late, so mucus isn't the primary issue. The problem is a catastrophic loss of gas exchange surface and elastic recoil. In chronic bronchitis (blue bloater), the primary pathology is in the bronchi and bronchioles—the conducting airways. The inflammation, gland enlargement, and mucus hypersecretion are the direct causes of obstruction and hypoxemia. The inflammatory mediators released in chronic bronchitis also contribute to systemic effects like weight loss (in some) or weight gain, and they promote the vascular changes leading to cor pulmonale.
The Role of Alpha-1 Antitrypsin Deficiency
It's crucial to note a key exception: Alpha-1 Antitrypsin Deficiency (AATD). This genetic disorder causes early-onset emphysema, typically in the lower lobes, and can affect non-smokers. Patients with AATD-related emphysema may not fit the classic "pink puffer" smoker profile and can sometimes present with more mucus production. This underscores that the blue bloater vs pink puffer model is a simplification, and individual variation is the rule.
Diagnostic Approach: Beyond the Nicknames
Modern diagnosis relies on spirometry, which measures lung function. The key metric is the Forced Expiratory Volume in 1 second (FEV1) and its ratio to Forced Vital Capacity (FVC). A post-bronchodilator FEV1/FVC < 0.70 confirms persistent airflow obstruction, diagnosing COPD. However, spirometry alone cannot definitively distinguish chronic bronchitis from emphysema or the phenotypes.
Additional Diagnostic Tools
- Imaging: A chest X-ray may show hyperinflation (flattened diaphragms) in emphysema and often appears normal in early chronic bronchitis. A CT scan is far superior, clearly showing emphysematous destruction (low-density areas) and airway wall thickening from chronic bronchitis.
- Arterial Blood Gas (ABG): This test directly measures PaO2 and PaCO2, helping to identify the hypoxemia and hypercapnia characteristic of the blue bloater phenotype.
- Clinical History: A detailed history of smoking (pack-years), occupational exposures, and symptom pattern (cough/sputum vs. dyspnea) is invaluable.
- Assessment of Comorbidities: Evaluating for cor pulmonale (via echocardiogram), polycythemia (CBC), and muscle wasting is essential, as these systemic manifestations differ between phenotypes.
Treatment Strategies: Tailoring Therapy to the Phenotype
While the foundational COPD treatments apply to all, understanding the dominant phenotype can guide more nuanced management, especially regarding oxygen therapy and exacerbation prevention.
Foundational COPD Management for All
- Smoking Cessation: The single most effective intervention to slow disease progression.
- Vaccinations: Annual influenza and pneumococcal vaccines are critical to prevent exacerbations.
- Pulmonary Rehabilitation: A comprehensive program of exercise, education, and breathing techniques (like pursed-lip breathing) that improves exercise tolerance and quality of life for all COPD patients.
- Pharmacotherapy: Includes bronchodilators (short-acting for rescue, long-acting for maintenance) like beta-agonists and anticholinergics, and inhaled corticosteroids for those with frequent exacerbations.
Phenotype-Specific Considerations
- For the "Pink Puffer" (Emphysema-Dominant):
- Focus on Dyspnea Relief: Long-acting bronchodilators are paramount to improve lung function and reduce air trapping.
- Lung Volume Reduction: In severe, upper-lobe-predominant emphysema, procedures like endoscopic lung volume reduction or surgical lung volume reduction can improve mechanics by allowing the diaphragm to descend and function more effectively.
- Nutritional Support: Due to the high metabolic cost of breathing and risk of cachexia, nutritional counseling and high-calorie supplements may be necessary.
- For the "Blue Bloater" (Chronic Bronchitis-Dominant):
- Focus on Mucus Clearance: Airway clearance techniques (e.g., postural drainage, positive expiratory pressure devices) and staying well-hydrated are important.
- Oxygen Therapy: Because of chronic hypoxemia, long-term oxygen therapy (LTOT) for ≥15 hours per day is often prescribed earlier and is a proven survival benefit.
- Exacerbation Prevention: The high sputum production makes them more susceptible to bacterial infections. Prophylactic antibiotics (like azithromycin) may be considered in select patients with frequent exacerbations, and aggressive treatment of infections is key.
- Managing Cor Pulmonale: Diuretics may be used to manage peripheral edema from right heart failure.
Prognosis and Disease Progression
The prognosis of COPD is variable and depends on the severity of airflow limitation (GOLD stage), presence of exacerbations, comorbidities, and phenotype. Historically, the "blue bloater" was thought to have a worse prognosis due to frequent exacerbations, hypoxemia, and cor pulmonale. The "pink puffer" might progress more insidiously but could reach a state of severe respiratory failure. However, this is an oversimplification. A patient with severe emphysema and profound hyperinflation can have a very poor quality of life and prognosis. The modern view is that frequent exacerbations—regardless of phenotype—are the strongest predictor of poor outcomes, including accelerated lung function decline, hospitalization, and mortality. The development of pulmonary hypertension and cor pulmonale significantly worsens prognosis in any phenotype.
Addressing Common Questions and Modern Perspectives
Q: Can someone be both a blue bloater and a pink puffer?
A: Absolutely. This is the most common scenario. Most COPD patients have a mixture of chronic bronchitis and emphysema. They might have a productive cough (bronchitic feature) but also be thin and breathless (emphysematous feature). The terms are best used as descriptive ends of a spectrum.
Q: Which is worse, blue bloater or pink puffer?
A: Neither is inherently "worse." They represent different challenges. The blue bloater battles chronic infection risk, hypoxemia, and heart strain. The pink puffer fights relentless dyspnea, hyperinflation, and gas exchange failure. Severity is determined by lung function tests (FEV1%), exacerbation history, and presence of comorbidities, not by which nickname fits best.
Q: Do these terms matter in modern medicine?
A: Yes, but in a evolved way. While doctors no longer rigidly categorize patients as one or the other, the concepts behind the terms remain clinically relevant. They remind clinicians to look for the dominant pathology—is the problem mostly mucus plugging (treat with mucolytics, airway clearance) or mostly alveolar destruction (treat with bronchodilators, consider lung volume reduction)?—and to screen for the specific complications associated with each (e.g., LTOT for hypoxemia, nutritional support for cachexia).
Q: Can lifestyle changes alter which "type" you are?
A: The underlying pathology is fixed, but symptoms and complications can be managed.Smoking cessation is non-negotiable and slows progression for both. Pulmonary rehabilitation improves efficiency for the pink puffer and builds strength for the blue bloater. Weight management is crucial—losing excess weight helps the blue bloater reduce cardiac workload, and gaining healthy weight (with protein) helps the pink puffer combat cachexia.
Conclusion: Moving Beyond the Nicknames to Personalized Care
The "blue bloater vs pink puffer" framework is a powerful historical tool that simplifies the complex pathology of COPD into two memorable archetypes. The chronic, mucus-filled airways and hypoxemia of the blue bloater contrast sharply with the destroyed alveoli, hyperinflation, and dyspnea of the pink puffer. Understanding this dichotomy illuminates why two patients with the same spirometry result can look and feel so different. It explains why one struggles with swollen ankles and a constant cough while another is thin, breathless, and purses their lips to walk.
However, the modern reality of COPD is one of spectrums and mixtures. Most patients exist somewhere in between, carrying features of both chronic bronchitis and emphysema. The true value of these classic descriptions today lies not in labeling patients, but in sharpening clinical thinking. It prompts the physician to ask: Is mucus obstruction or alveolar destruction the dominant driver of this patient's symptoms? Are they hypoxemic? Are they developing right heart strain? Is cachexia a concern?
Ultimately, whether a patient leans toward blue bloater, pink puffer, or a blend of both, the path forward is the same: a commitment to smoking cessation, evidence-based pharmacotherapy, the transformative power of pulmonary rehabilitation, vigilant vaccination and infection control, and the timely use of oxygen therapy when indicated. The goal is not to fit into a nostalgic nickname, but to achieve the best possible quality of life and slow the disease's march through truly personalized, comprehensive care. If you or a loved one shows symptoms of COPD—persistent cough, shortness of breath, wheezing—consult a healthcare provider. A simple spirometry test can be the first step toward understanding your specific form of COPD and accessing the targeted treatments that can make all the difference.