Caput Succedaneum Vs Cephalohematoma: Decoding Your Newborn's Head Bump
Is that swelling on your baby's head after birth a cause for alarm or a normal part of the journey? The moment you meet your newborn, every detail matters. You count fingers and toes, marvel at tiny features, and then perhaps your eyes land on a soft, squishy bump or a firm, raised area on their scalp. Your heart skips a beat. Two of the most common reasons for this are caput succedaneum and cephalohematoma—terms that sound intimidating but describe very different, usually benign, birth-related swellings. Understanding the caput succedaneum vs cephalohematoma distinction is crucial for every new parent, providing peace of mind and clarity on when to simply watch and wait and when to consult your pediatrician.
This comprehensive guide will walk you through everything you need to know. We'll define each condition in plain language, explore their distinct causes and appearances, compare their symptoms and potential complications side-by-side, and outline the standard treatment pathways. By the end, you'll be equipped with the knowledge to recognize these common neonatal findings, understand their typical course, and advocate effectively for your little one's health.
What Exactly Is Caput Succedaneum?
Let's start by demystifying the first term. Caput succedaneum (pronounced kuh-POOT suk-uh-DAY-nee-um) is a Latin phrase that essentially means "head that has been substituted" or "head that has fallen forward." In medical terms, it refers to a edema, or fluid accumulation, in the scalp's soft tissues—specifically, the skin and the subcutaneous layer just beneath it.
The Mechanism: Pressure and Fluid Shift
This swelling occurs before birth, during the labor and delivery process. As the baby's head descends through the birth canal, it is subjected to significant pressure against the mother's pelvic bones and the cervix. This pressure acts like a squeeze, temporarily compressing the scalp and forcing fluids (primarily serous fluid, which is a thin, watery plasma) out of the blood vessels and into the surrounding interstitial tissues. Think of it like pressing on a wet sponge; the water moves to the area of least resistance.
A key characteristic of caput succedaneum is that it crosses suture lines. The sutures are the fibrous joints between the bony plates of an infant's skull. Because the fluid is located in the soft tissue above the skull bones, it is not confined by these sutures and can easily spread over a large area, sometimes crossing the midline of the head. It is typically soft, boggy, and poorly defined, blending gradually into the surrounding normal scalp. It is present at birth and is often more pronounced in babies born after a long, difficult labor or with the assistance of a vacuum extractor or forceps, though it can occur in any vaginal delivery.
Common Presentation and Course
The swelling from caput succedaneum is usually noticeable immediately after birth. It can feel like a water-filled balloon under the skin. The skin over the area might look stretched and shiny but is typically its normal color, though it can sometimes have a slight bruise-like discoloration if small capillaries were also damaged. The most important thing to remember is that caput succedaneum is almost always harmless and self-resolving. The body simply reabsorbs the extra fluid over the first few days of life, with the swelling typically diminishing significantly within 24-48 hours and disappearing completely within a week or so. No specific medical intervention is required.
Understanding Cephalohematoma: A Different Kind of Swelling
Now, let's turn to cephalohematoma (pronounced sef-uh-loh-hee-MAT-oh-muh), a term derived from Greek roots meaning "head" and "a blood collection." This condition is fundamentally different from caput succedaneum in both its location and its composition.
The Mechanism: Bleeding Between Layers
A cephalohematoma is a collection of blood that accumulates between the skull bone and the periosteum, which is the tough, fibrous membrane that tightly covers the outer surface of the bone. This bleeding originates from the tiny blood vessels that run along the sutures, which are often torn during the mechanical stress of delivery. Because the blood is trapped under the periosteum, it is strictly confined by the suture lines of the skull. It cannot cross a suture. This creates a very distinctive, well-defined, raised ridge that follows the contour of the underlying skull bone, often limited to one bone (like the parietal bone on the side of the head).
The blood collection is initially liquid but will gradually clot and then organize. Over weeks, the body breaks down the clotted blood (a process involving hemoglobin breakdown) and slowly reabsorbs it. This is a much slower process than fluid reabsorption. Cephalohematomas are also more common with instrumental deliveries (vacuum, forceps) and with larger babies or a firstborn (where the maternal tissues may be less "giving").
The "Rock-Hard" Feel and Gradual Resolution
At birth, a cephalohematoma may feel firm or even hard, like a rubbery or bony bump, because it is a contained pool of clotted blood sitting on the skull. The overlying skin is usually normal in color and temperature. A critical point of confusion: a cephalohematoma does not present as a soft, squishy swelling; it has a definite, raised edge. The swelling may not be immediately obvious at birth but can grow larger over the first few days as more blood seeps into the collection—a phenomenon called "delayed expansion." Parents often notice it getting more prominent on day 2 or 3.
The resolution timeline is the second major difference. While caput succedaneum fades in days, a cephalohematoma can take weeks to months to fully disappear. The average duration is 6-8 weeks, but larger collections can take 3 months or more. During this time, the bump will gradually soften and shrink. As the blood breaks down, the skin over the area may turn yellowish or greenish (like a bruise), which is a normal part of the healing process.
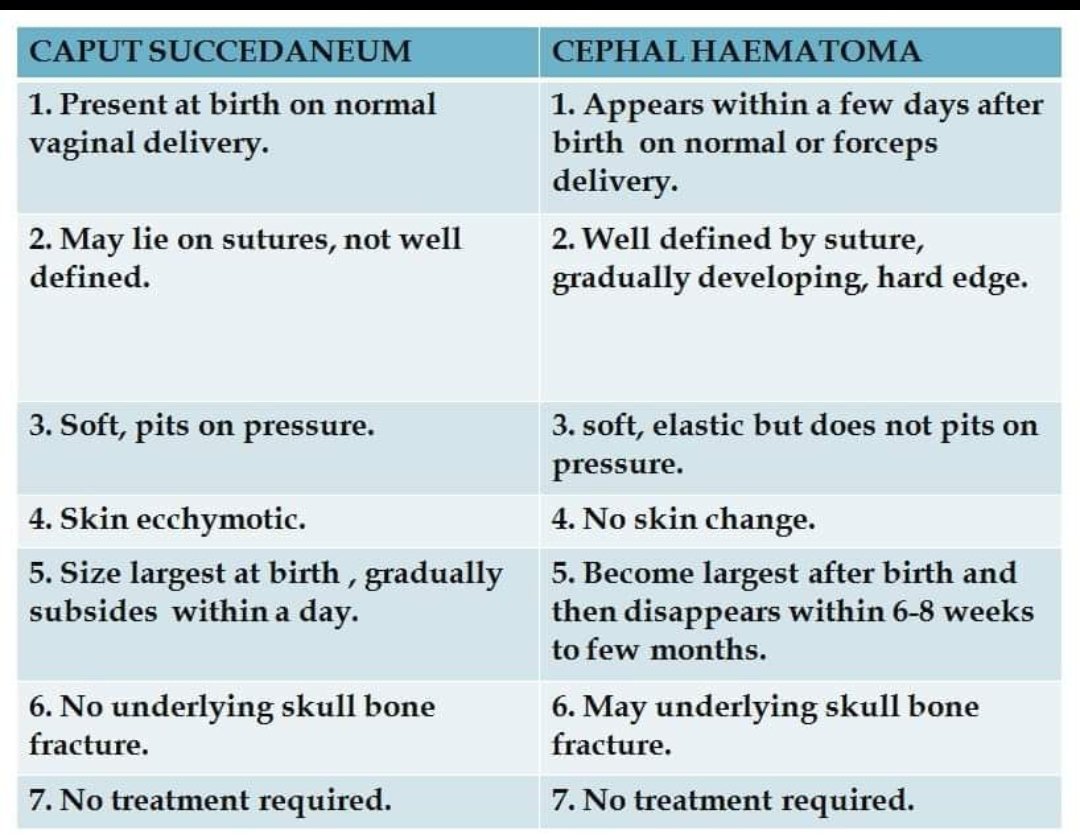
Side-by-Side Showdown: Caput Succedaneum vs Cephalohematoma
To make the differences crystal clear, let's put them head-to-head in a direct comparison.
| Feature | Caput Succedaneum | Cephalohematoma |
|---|---|---|
| What is it? | Edema (fluid) in scalp tissues | Hematoma (blood) between skull & periosteum |
| Location | Above the skull bone, in soft tissue | Under the periosteum, on the skull bone |
| Crosses Sutures? | YES – spreads across suture lines | NO – confined by suture lines |
| Feel at Birth | Soft, boggy, poorly defined | Firm, rubbery, well-defined ridge |
| Onset | Present at birth | May grow for 1-3 days after birth |
| Color/Skin | Usually normal; may be slightly bruised | Skin is normal; later shows bruise colors |
| Primary Cause | Pressure from birth canal | Rupture of blood vessels along sutures |
| Contents | Serous fluid (watery plasma) | Clotted & liquefying blood |
| Resolution Time | Days (typically < 1 week) | Weeks to Months (6-12+ weeks) |
| Complication Risk | Very low | Higher – risk of jaundice, calcification |
The Critical "Crosses Sutures" Rule
If you can remember one thing from this caput succedaneum vs cephalohematoma comparison, it's this: Does the swelling cross the soft spot (fontanelle) or the suture lines on your baby's skull? If you can gently feel a smooth, continuous swelling that goes over a suture or the midline, it is almost certainly caput succedaneum. If you feel a distinct, hard edge that stops abruptly at a suture line, it is almost certainly a cephalohematoma. This is the single most reliable visual and tactile clue for parents and doctors alike.
Potential Complications: What to Watch For
While both conditions are usually benign, it's important to be aware of potential, albeit less common, complications, especially with cephalohematoma.
With Caput Succedaneum
Complications are exceedingly rare. The primary concern is if the edema is extremely extensive, which is unusual. The main "complication" is parental anxiety, which is completely understandable but typically unfounded given the benign and fleeting nature of this swelling.
With Cephalohematoma
The risks are more significant due to the presence of a large volume of broken-down blood (bilirubin) in the system.
- Hyperbilirubinemia (Jaundice): This is the most common complication. As the body breaks down the collected blood, it releases bilirubin, a yellow pigment. A large cephalohematoma can contribute to a higher bilirubin load, potentially worsening newborn jaundice. This may require more frequent monitoring and, in some cases, phototherapy (special blue light treatment) to prevent bilirubin from reaching dangerous levels.
- Calcification or "Bony" Hardening: In about 2-5% of cases, especially with very large or long-standing hematomas, the blood collection can calcify. This means calcium deposits form in the organizing clot, leading to a permanent, hard, bony-like ridge on the skull. This cephalohematoma calcification is a cosmetic concern that does not affect brain development but may be noticeable. It often resolves slowly over a year or more, but in rare persistent cases, surgical removal might be considered for cosmetic reasons after the child is older.
- Infection (Very Rare): If the skin over the hematoma is broken, bacteria could enter. Signs include increasing redness, warmth, swelling, pus, or fever.
- Anemia: Extremely large hematomas can cause a significant loss of blood volume into the collection, potentially leading to anemia. This is monitored by checking the baby's hemoglobin levels if the hematoma is very large.
Treatment and Management: What Should You Do?
The management philosophy for these two conditions is a perfect illustration of "watchful waiting" versus active monitoring.
For Caput Succedaneum
Treatment: None. The only "treatment" is time and gentle care.
- Do: Keep the area clean during baths. No special massage or manipulation is needed. The swelling will fade on its own.
- Do Not: Press on it, try to "drain" it, or apply any creams or ointments unless directed by a doctor. It is not a cyst or abscess; it's just fluid.
- Follow-up: No specific follow-up is required for the swelling itself. Your baby's routine pediatric visits are sufficient.
For Cephalohematoma
Treatment: Primarily observation and monitoring for jaundice.
- Do Not: Palpate or massage it aggressively. Do not attempt to aspirate (drain) it. Historically, doctors sometimes drained them, but this is now strongly discouraged due to high risks of infection, re-accumulation, and calcification. The body is best at reabsorbing it on its own.
- Do:
- Monitor Size: Gently feel the edges daily. Note if it seems to be getting significantly larger after the first few days (delayed expansion is normal, but rapid growth is not).
- Watch for Jaundice: This is the most important action. Look for yellowing of the skin, starting on the face and moving down the chest, abdomen, and legs. Check the whites of the eyes. Ensure your baby is feeding well to promote hydration and bowel movements, which help excrete bilirubin. Your pediatrician will likely check bilirubin levels more frequently for the first 1-2 weeks.
- Document: Take a clear photo on day 1, day 3, and day 7 to track its size and any color changes for your doctor.
- Follow-up: Your pediatrician will want to examine the hematoma at regular intervals (e.g., 1 week, 2 weeks, 1 month) to ensure it is slowly shrinking and not showing signs of infection or concerning calcification.
When to Call the Doctor: Red Flags
For both conditions, you should contact your pediatrician promptly if you notice:
- Rapid increase in size of the swelling after the first 3-4 days.
- Signs of infection: Increasing redness, warmth, swelling, or pus at the site. Fever (temperature above 100.4°F or 38°C rectally in a newborn).
- Signs of worsening jaundice: Yellowing that spreads quickly to the legs or palms/soles, poor feeding, lethargy, high-pitched crying, or arching of the back.
- The baby seems unusually fussy, irritable, or has a seizure. (This is very rare and not typical of either condition alone, but must be ruled out if other serious issues like intracranial bleed are a concern).
- You have any doubt or anxiety. It is always okay to call your doctor with questions. A quick exam can provide immense peace of mind.
Prevention and Risk Factors
While you cannot completely prevent these birth-related occurrences, understanding the risk factors can provide context.
- Common Risk Factors for Both:
- Prolonged or difficult labor (especially second stage).
- Instrumental delivery (vacuum extraction, forceps).
- Large baby (macrosomia).
- First pregnancy (less flexible maternal tissues).
- Multiple gestation (twins, etc.).
- Maternal diabetes (can lead to larger babies).
- Specific to Cephalohematoma: The risk is more strongly tied to the direct mechanical forces on the skull during delivery, making instrumental deliveries the most significant modifiable risk factor. The skill and technique of the delivering clinician play a role.
It's vital to understand that the presence of a caput succedaneum or cephalohematoma is not a sign of poor parenting or medical negligence. They are common, mechanical consequences of the birthing process, a testament to the intense journey a baby undertakes to enter the world. The vast majority resolve without any long-term effects.
Addressing Parental Concerns: FAQs
Q: Is a cephalohematoma brain damage?
A: Absolutely not. A cephalohematoma is a collection of blood outside the skull, between the skull bone and its covering membrane. It is a subperiosteal hemorrhage, not an intracranial hemorrhage (bleeding inside the skull). The baby's brain is protected by the skull and is not affected by the hematoma itself. The concern is the blood breakdown products (bilirubin) and, rarely, cosmetic calcification.
Q: Will my baby need surgery?
A: For the vast majority of cases, no surgery is ever needed. The standard of care is conservative management. Surgery to remove the calcified shell of a healed hematoma is a rare, last-resort cosmetic procedure performed years later, if at all.
Q: Can I feel the "soft spot" (fontanelle) through the swelling?
A: With caput succedaneum, the swelling is so diffuse and soft that you can usually still feel the underlying fontanelle and sutures. With a cephalohematoma, the firm collection sits on top of the skull bone, so the fontanelle will feel normal and separate from the hard, raised edge of the hematoma.
Q: Does breastfeeding help?
A: Yes! Frequent, effective breastfeeding ensures your baby is well-hydrated and has regular bowel movements. This is crucial for helping the body excrete bilirubin, thereby reducing the risk of significant jaundice from a large cephalohematoma.
Q: Will it leave a scar?
A: Neither condition leaves a scar on the skin. The skin is intact. A large cephalohematoma that calcifies may leave a palpable, permanent ridge under the skin, but the skin surface itself remains normal.
Conclusion: Knowledge is the Best Soother
The discovery of a bump on your newborn's head can be a moment of sheer panic. But armed with the clear distinctions between caput succedaneum and cephalohematoma, that panic can transform into informed, calm observation. Remember the golden rule: fluid crosses sutures (caput succedaneum), blood does not (cephalohematoma).
Caput succedaneum is a fleeting, soft edema that vanishes in days. Cephalohematoma is a firmer, contained blood collection that takes weeks to months to fade, with the primary medical consideration being its potential contribution to newborn jaundice. Both are common, almost always benign relics of the birth process, not indicators of underlying brain injury.
Your role as a parent is to be a keen observer, a diligent monitor for jaundice, and a proactive communicator with your pediatrician. Take those photos, track the changes, and ask your questions. In the overwhelming early days of parenthood, this is one area where you can be confident. That bump is likely just a temporary badge of honor from a job well done—your baby's successful entrance into the world. With time, patience, and routine medical care, it will disappear, leaving behind only the memory of a worry and the joy of a healthy, growing child.