Is Broken The Same As Fracture? The Critical Difference Every Patient Must Know
When you hear "your bone is broken" versus "you have a fracture," do you assume they mean two different things? You’re not alone. This common question—is broken the same as fracture—plagues millions of people after an injury, creating confusion at a time of pain and stress. The short answer might surprise you: in everyday language, they mean the same thing. But in the precise world of medicine, the word "fracture" carries more nuance, specificity, and diagnostic weight. Understanding this distinction isn't just semantics; it directly impacts how you communicate with doctors, interpret your diagnosis, and follow your treatment plan. This guide will dismantle the myths, clarify the terminology, and empower you with the knowledge to navigate bone injuries with confidence.
Understanding the Basics: Definitions and Common Usage
The Layperson's Perspective: "Broken" as a Universal Term
For most of us, a broken bone is a broken bone. It’s the simple, powerful, and slightly alarming term we use when we hear that tell-tale crack or experience severe pain after a fall. "My arm is broken!" is a cry for help everyone understands. This term is emotionally resonant and universally accessible. It conveys a clear sense of severity and urgency. In casual conversation, at a playground, or in a frantic call to a family member, "broken" is the undisputed champion of bone injury vocabulary. Its strength lies in its absolute clarity—there is no middle ground. Something is either broken or it is not.
The Medical Perspective: "Fracture" as the Clinical Standard
Step into a doctor's office or an emergency room, and the language shifts. You will almost certainly hear the term fracture. This is the preferred, precise terminology in all medical literature, diagnosis codes (like ICD-10), and clinical notes. A fracture is defined as a partial or complete break in the continuity of a bone. The word itself comes from the Latin fractura, meaning "a breach" or "a break." Its use signals that the diagnosis was made through clinical assessment, often confirmed by imaging like an X-ray, CT scan, or MRI. "Fracture" is the umbrella term under which all specific types of bone breaks are classified.
So, Are They Interchangeable?
Here is the crucial synthesis: Yes, for all practical intents and purposes, a "broken bone" is a "fracture." If you are told you have a fracture, you have a broken bone. If you are told your bone is broken, you have a fracture. The confusion arises because "fracture" is not a milder term; it is simply the correct medical term. Think of it like "myocardial infarction" versus "heart attack." They describe the same catastrophic event, but one is the formal clinical label. The key takeaway is that the severity is contained not in the word "broken" or "fracture" itself, but in the specific type and classification of that fracture, which your healthcare provider will determine.
The Spectrum of Severity: It's Not All "Broken" Equal
This is where the real importance of medical terminology shines. Not all fractures are created equal, and the specific descriptor tells the entire story of the injury's complexity and required treatment.
Simple (Closed) vs. Compound (Open) Fractures
This is the most fundamental classification. A simple or closed fracture means the bone has broken, but the skin remains intact. The damage is confined to the bone and surrounding tissues. This is the most common type. Conversely, a compound or open fracture is a medical emergency. Here, the broken bone pierces the skin, or a wound penetrates down to the broken bone. This exposes the deep tissue and bone to the external environment, creating a high risk for severe infection. The treatment protocols, urgency, and recovery timelines differ dramatically between these two types, regardless of whether you call them "broken" or "fractured."
Stable vs. Unstable Fractures
Stability refers to whether the broken bone fragments are likely to move out of alignment. A stable fracture is one where the bone pieces remain in a relatively good position. It is often treated conservatively with a cast or splint. An unstable fracture has fragments that can shift easily, jeopardizing proper healing. These frequently require surgical intervention with plates, screws, or rods to stabilize the bone. A simple "broken wrist" could be a stable, minimally displaced fracture or an unstable, comminuted (shattered) fracture requiring surgery—a world of difference in recovery.
Complete vs. Incomplete Fractures
A complete fracture means the bone is broken all the way through. An incomplete fracture does not extend through the entire bone. This is common in children, whose bones are more flexible. A greenstick fracture (like a green twig) bends and cracks on one side only. A buckle or torus fracture involves compression of the outer bone layer without a full break. These distinctions are critical for pediatric orthopedics and influence casting techniques and healing time.
Why Doctors Say "Fracture": The Clinical and Diagnostic Imperative
Precision in Communication
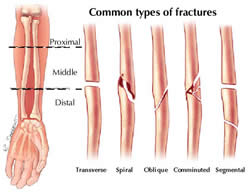
The medical world thrives on unambiguous language. Saying "fracture" immediately places the injury into a standardized diagnostic category. It prompts specific questions: Is it transverse, oblique, or spiral? Is it displaced? Is it intra-articular (involving a joint)? These descriptors, attached to the word "fracture," form a complete clinical picture. "Broken" is a lay summary; "fracture" is the entry point into a detailed diagnostic algorithm.
Coding, Billing, and Research
Medical records, insurance claims, and scientific studies rely on precise terminology. The term "fracture" is linked to specific ICD-10 codes (e.g., S52.501A for an unspecified fracture of the lower end of the right radius, initial encounter for closed fracture). This coding system is the backbone of healthcare administration, research epidemiology, and public health statistics. Using "broken" in a formal record would be insufficient and unprofessional.
Setting Patient Expectations
When a doctor says, "You have a non-displaced transverse fracture of the distal radius," they are providing a wealth of information. You know the bone (radius), the location (distal, or wrist), the pattern (a clean, horizontal line), and the alignment (non-displaced, meaning pieces are still in place). This immediately informs the likely treatment (casting) and prognosis. "Your wrist is broken" lacks this crucial detail and can cause unnecessary anxiety or false assumptions.
Treatment Pathways: How the Label Influences Your Care
The management of a bone injury is dictated by the fracture's characteristics, not the word used to describe it. However, understanding the medical label helps you understand your treatment.
Conservative Management: Casting and Splinting
For many stable, closed, non-displaced fractures, the treatment is immobilization. This involves a cast, splint, or brace to hold the bone fragments in perfect position while the body's natural healing processes—involving osteoblasts (bone-building cells) and a soft callus that hardens—do their work. The duration can range from 3 weeks for a child's buckle fracture to 8-12 weeks for an adult's tibial fracture. Understanding that your "break" is a "stable, closed fracture" explains why you aren't going straight to surgery.
Surgical Intervention: Open Reduction and Internal Fixation (ORIF)
For displaced, unstable, intra-articular, or open fractures, surgery is often necessary. The gold standard procedure is ORIF. Surgeons make an incision (open reduction), realign the bone fragments to their anatomical position, and then fix them permanently with internal hardware like plates and screws or intramedullary nails. This provides rigid stability, allowing for earlier motion and often a better functional outcome, especially for joint fractures. Knowing you have an "unstable, displaced fracture" explains the surgical recommendation.
Rehabilitation and The Healing Timeline
Healing is a biological process, not a calendar event. The fracture healing timeline involves inflammatory, reparative, and remodeling phases. Factors like age, nutrition (calcium and vitamin D intake), smoking status, and blood supply dramatically affect healing. A "simple fracture" in a healthy 20-year-old may heal in 6 weeks, while a complex fracture in a 70-year-old with osteoporosis may take 4-6 months. Your treatment plan—including physical therapy to regain strength and range of motion—is tailored to your specific fracture type and individual health profile.
Debunking Common Myths and Misconceptions
Myth 1: "A Fracture is Less Serious Than a Break"
This is the most pervasive and dangerous myth. As established, they are synonymous in terms of bone discontinuity. A "hairline fracture" (often a stress fracture) can be incredibly painful and require months of rest, while a "simple break" in a good location might heal uneventfully in a cast. Severity is defined by the fracture pattern, location, and displacement, not the word used.
Myth 2: "If I Can Move It, It's Not Broken"
False. The ability to move a limb does not rule out a fracture. Sprains, strains, and minor fractures can all allow for some movement. The classic signs of a fracture are pain, swelling, deformity, bruising, and inability to bear weight or use the limb normally. However, some fractures (like stress fractures) present with only vague pain that worsens with activity. When in doubt, always seek medical evaluation and an X-ray.
Myth 3: "You Can Always Tell When a Bone is Broken by the Sound"
While a distinct "crack" or "snap" is common in traumatic fractures, it is not universal. Many fractures, especially stress fractures or those in older adults with osteoporotic bone, occur with minimal or no audible sound. Do not rely on sound as a diagnostic tool.
Myth 4: "Bones Heal Stronger After a Break"
This is a partial truth wrapped in a misconception. The healed bone, after remodeling over 1-2 years, can return to its original strength. It does not become inherently "stronger" or thicker than before. The area of healing may be slightly bulkier initially (a "callus"), but it remodels to its original shape. The real "strength" comes from following rehabilitation to rebuild the surrounding muscles, tendons, and ligaments that support the bone.
Actionable Tips: What To Do If You Suspect a Fracture
- Seek Immediate Medical Attention for Open Fractures, Severe Deformity, or Numbness. These are emergencies. Control bleeding with clean pressure, immobilize the limb, and get to an ER.
- For Suspected Closed Fractures, Follow R.I.C.E. Initially:Rest the injured area. Apply Ice packs (wrapped in a towel) for 15-20 minutes every 1-2 hours to reduce swelling. Use Compression with an elastic bandage (not too tight). Elevate the limb above heart level if possible.
- Immobilize the Area. Use a makeshift splint (like a rolled-up magazine or board) and soft padding to prevent movement. Do not try to realign a visibly deformed bone.
- Get a Professional Diagnosis. An X-ray is the standard first step. In some cases (like wrist or foot fractures), multiple views are needed. For suspected stress fractures or complex areas, a CT or MRI may be ordered.
- Follow Your Treatment Plan Meticulously. Whether it's a cast, boot, or post-surgery protocol, adherence is non-negotiable for proper healing. Understand your weight-bearing status: non-weight bearing (NWB), partial weight bearing (PWB), or weight bearing as tolerated (WBAT).
- Attend All Follow-Up Appointments. Doctors monitor healing with follow-up X-rays. They also manage cast changes and assess for complications like compartment syndrome (a surgical emergency from pressure buildup) or non-union (failure of the bone to heal).
- Prioritize Nutrition and Lifestyle. Support your body's healing with adequate protein, calcium, vitamin D, and vitamin C. Avoid smoking and excessive alcohol, which severely impair bone healing.
The Bigger Picture: Bone Health and Prevention
Understanding fracture terminology is part of a larger conversation about skeletal health. A fracture, especially from a low-impact fall (a fragility fracture), can be a sentinel event indicating underlying osteoporosis or osteopenia. If you are over 50 (women) or 65 (men) and sustain a fracture, it is crucial to discuss bone density testing (DEXA scan) with your doctor. Prevention strategies—weight-bearing exercise (walking, lifting weights), adequate calcium and vitamin D intake, fall prevention strategies at home, and medication when indicated—are paramount to avoiding future fractures.
Conclusion: Knowledge is Your Best Medicine
To directly answer the core question: Is broken the same as fracture? In the context of a bone injury, yes, they refer to the same fundamental event—a discontinuity in the bone structure. However, the term "fracture" is the medically accurate, precise, and universally accepted label in healthcare. The true meaning and urgency of your injury are not found in the choice between these two words, but in the specific classification that follows: displaced, compound, stable, or stress. This classification dictates your treatment, your recovery timeline, and your future prevention strategies.
When you hear "fracture," don't panic because it sounds clinical. Instead, ask for the specifics: "What type of fracture is it?" "Is it displaced?" "Is it stable?" "What is the treatment plan?" By moving from the general question of "broken vs. fracture" to the specific details of your fracture, you transform from a passive patient into an active, informed participant in your own healing journey. In the realm of bone injuries, precise language isn't just semantics—it's the foundation of effective care, optimal recovery, and long-term skeletal resilience. Arm yourself with this knowledge, ask the right questions, and partner with your healthcare team for the best possible outcome.