The Mesenteric Ileal Branch In Dogs: A Vital Vascular Highway You Need To Know About
Have you ever wondered what keeps your dog's intestines alive and functioning? Beneath the furry surface lies a complex network of blood vessels, each playing a critical role in health. Among these, a specific artery—the mesenteric ileal branch—is a true lifeline for a crucial part of the digestive system. Understanding this tiny but mighty vessel is not just for veterinarians; it's essential knowledge for any dedicated dog owner who wants to advocate for their pet's well-being. This comprehensive guide will navigate the anatomy, significance, and clinical importance of the mesenteric ileal branch in dogs, empowering you with insights that could make all the difference in a health crisis.
The mesenteric ileal branch is a terminal artery originating from the superior mesenteric artery, itself a major branch of the aorta. Its sole purpose is to supply oxygen-rich blood to the ileum, the final segment of the small intestine. This artery's health is directly tied to the viability of the intestinal tissue it feeds. Compromise this blood flow, even slightly, and the consequences can range from mild discomfort to life-threatening intestinal necrosis. Throughout this article, we will explore this vessel's journey, its vulnerabilities, and what modern veterinary medicine does to protect it. Whether you're facing a surgical decision or simply curious about canine anatomy, this deep dive will illuminate a critical, often overlooked, component of your dog's internal world.
What Exactly is the Mesenteric Ileal Branch in Dogs?
Defining the Artery and Its Role
The mesenteric ileal branch is a specific, named artery within the canine abdominal vasculature. It is one of the final divisions of the superior mesenteric artery (SMA), which itself branches off the abdominal aorta just behind the kidney. Think of the SMA as a main highway and the mesenteric ileal branch as a critical exit ramp leading directly to the ileum. Its primary, non-negotiable function is vascular perfusion—delivering a constant stream of oxygen and nutrients to the ileal wall and its microscopic villi, which are responsible for nutrient absorption. Without this precise blood supply, the cells of the ileum cannot produce energy, leading to rapid cell death and tissue breakdown. This artery's territory is highly specific, making it a key landmark in both health and disease.
How It Differs from Other Mesenteric Vessels
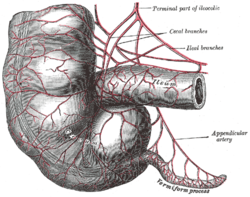
The canine mesenteric system is a branching tree. The SMA gives rise to several important branches before the ileal branch, including the jejunal arteries (supplying the mid-small intestine) and the ileocolic artery (which often supplies the ileum's very end and the cecum). The mesenteric ileal branch is typically the most distal of these SMA branches, dedicated almost exclusively to the mid to distal ileum. This specificity is crucial for surgeons. Unlike the more robust jejunal arteries which have significant anastomoses (connections) with each other, the ileal branch can be more solitary in its path. This "end-artery" characteristic means it has less backup blood supply from neighboring vessels, making its integrity even more vital and its occlusion more dangerous for that specific intestinal segment.
Anatomical Journey: From Origin to Destination
Where It Begins: The Superior Mesenteric Artery
To understand the ileal branch, you must first locate its parent vessel. The superior mesenteric artery arises from the abdominal aorta's ventral surface, typically at the level of the celiac artery (which supplies the stomach and liver). In dogs, the SMA is a powerful, pulsatile vessel that immediately begins branching as it courses caudally (toward the tail) along the dorsal abdominal wall. It is encased within the mesentery, the fold of tissue that suspends the intestines like a hammock. The SMA's first branches are usually the pancreaticoduodenal arteries, followed by multiple jejunal arteries. After these, the pattern becomes more variable, but the mesenteric ileal branch consistently emerges as one of the last major divisions before the SMA terminates.
The Path It Takes Through the Canine Abdomen
After branching from the SMA, the mesenteric ileal branch embarks on a precise course within the mesentery proper. It travels within the connective tissue, following the mesenteric root—the point where the mesentery attaches to the dorsal abdominal wall. Its path is generally directed toward the antimesenteric border of the ileum (the side opposite the mesenteric attachment). Along its journey, it gives off smaller vasa recta (straight arteries) that penetrate the intestinal wall at right angles. These vasa recta form a delicate arcade within the submucosa and mucosa, creating a fine network that perfuses every cell. The artery's length and exact branching pattern can vary slightly between individual dogs and breeds, but its destination is constant: the ileal wall.
Where It Ends: Supplying the Ileum and Beyond
The terminal arterioles of the mesenteric ileal branch end in a capillary bed within the mucosa and submucosa of the ileum. This is the site of the famous intestinal villi and microvilli, the finger-like projections where the magic of nutrient absorption occurs. A healthy blood flow here is essential for transporting absorbed amino acids, sugars, and fatty acids away from the gut into the portal circulation. In some dogs, the ileal branch may have a small anastomosis with the ileocolic artery near the ileocecal junction (where the small and large intestines meet), providing a minor backup route. However, this connection is often insufficient to save the mid-ileum if the primary ileal branch is completely blocked, highlighting its status as a critical, relatively isolated supply line.
Why This Tiny Artery Matters: Clinical Significance
The Lifeline for Intestinal Health
The clinical significance of the mesenteric ileal branch cannot be overstated. It is the sole provider of oxygen for a significant portion of the small intestine's absorptive surface. Ischemia—a lack of blood flow—to this area leads to rapid compromise. Within minutes, intestinal epithelial cells begin to die. Within hours, the mucosal barrier breaks down, allowing bacteria and toxins from the gut lumen to translocate into the bloodstream, causing sepsis and systemic inflammatory response syndrome (SIRS). This cascade is a primary reason why acute abdominal pain in dogs is such a medical emergency. The location of the pain can sometimes hint at the vascular territory involved; pain localized to the mid-abdomen may implicate the SMA and its ileal branch.
Surgical Implications: A Surgeon's Delicate Balance
For veterinary surgeons, the mesenteric ileal branch is a constant consideration during any abdominal procedure involving the small intestine—be it an intestinal resection for cancer or foreign body removal, a spay (ovariohysterectomy), or even a biopsy. The goal is always to preserve adequate blood supply to the remaining intestine. During an intestinal resection, the surgeon must identify and ligate (tie off) the mesenteric ileal branch at a point proximal (closer to the SMA) to the diseased segment. This ensures the remaining distal ileum retains a healthy blood supply from collateral flow, if present, and prevents anastomotic breakdown—where the surgical connection between intestinal ends fails due to poor healing from lack of blood. A single misjudged ligation can lead to catastrophic post-operative necrosis.
What Happens When It's Compromised?
Compromise of the mesenteric ileal branch can occur through several mechanisms, each with devastating effects. Thrombosis (a clot forming within the artery) or embolism (a clot traveling from elsewhere and lodging in the artery) causes sudden, complete occlusion. The result is acute mesenteric ischemia, characterized by severe, out-of-proportion pain, vomiting (often bloody), diarrhea, and rapid deterioration. Trauma, such as from a bite wound or blunt force, can lacerate or compress the vessel. Iatrogenic injury during surgery, though rare with experienced hands, is a known risk. Vasculitis (inflammation of the vessel wall) from autoimmune disease or infection can narrow the lumen over time, causing chronic, intermittent pain and malabsorption. The common endpoint of all these is intestinal necrosis, which is often fatal without immediate, aggressive intervention.
Common Pathologies Affecting the Mesenteric Ileal Branch
Thrombosis and Embolism: Silent Killers
Arterial thrombosis and embolism are the most acute threats. In dogs, emboli often originate from cardiac disease like atrial fibrillation or endocarditis, where clots form in the heart and are pumped into the systemic circulation. A clot the size of the ileal branch's lumen can completely plug it. Thrombosis can also form in situ due to underlying endothelial damage from conditions like pancreatitis (inflammation of the pancreas, which sits near the SMA) or hypercoagulable states. The clinical presentation is classic: a dog with a known cardiac condition suddenly collapses with abdominal pain. Diagnosis is notoriously difficult, as standard bloodwork may only show subtle signs like a mild leukocytosis or elevated lactate. Time is the ultimate enemy; irreversible damage can occur in as little as 4-6 hours of complete occlusion.
Traumatic Injury and Iatrogenic Damage
Blunt abdominal trauma, such as from a dog fight or being hit by a car, can cause shearing forces that rupture the mesenteric vessels. The mesenteric ileal branch, being relatively fixed within the mesentery, is susceptible. Penetrating wounds (bite wounds, gunshot wounds) can directly sever it. Iatrogenic injury refers to damage caused during veterinary surgery. While routine procedures like spays are generally safe, a surgeon working in the caudal abdomen must be acutely aware of the mesenteric root. An overly aggressive retraction or an errant suture can compromise this vessel. Such injuries might not be apparent intra-operatively but can manifest 24-48 hours post-op as the dog deteriorates with signs of peritonitis and sepsis, a dreaded complication.
Inflammatory Conditions and Vasculitis
Immune-mediated vasculitis can target the mesenteric arteries, including the ileal branch. Conditions like systemic lupus erythematosus (SLE) or polyarteritis nodosa can cause inflammation, thickening, and narrowing of the arterial wall. This leads to chronic mesenteric ischemia, a harder-to-diagnose condition where blood flow is progressively reduced. Symptoms are often vague: intermittent vomiting, decreased appetite, weight loss, and chronic abdominal pain that waxes and wanes. Dogs may appear to have "sensitive stomachs." Pancreatitis is another critical link; the inflamed pancreas can directly irritate and compress the adjacent SMA and its branches, potentially leading to secondary thrombosis or spasm in the mesenteric ileal branch, exacerbating the intestinal component of the disease.
How Vets Diagnose Issues with This Artery
Ultrasound: The First Line of Defense
Abdominal ultrasound is the primary, non-invasive diagnostic tool for evaluating mesenteric vessels. A skilled sonographer can use Doppler ultrasonography to assess blood flow velocity and direction in the superior mesenteric artery and its major branches, including the ileal branch. Key findings include: absence of flow (indicating occlusion), turbulent flow (suggesting a stenosis or thrombus), or reduced flow velocity. The ultrasound also evaluates the intestinal wall thickness and mucosal pattern. Thickened, hypoechoic (dark) bowel walls with loss of the normal layered structure are highly suggestive of ischemic bowel disease. While identifying the tiny, distal mesenteric ileal branch itself can be challenging, its parent vessel's flow and the condition of the ileal wall provide strong indirect evidence.
Advanced Imaging: CT and MRI Angiography
When ultrasound is inconclusive, computed tomography angiography (CTA) is the gold standard. This involves injecting an iodine-based contrast agent intravenously and performing a rapid, high-resolution CT scan. The software can reconstruct 3D images of the abdominal vasculature, allowing the radiologist to trace the superior mesenteric artery down to its ileal branch and visually identify any blockages, narrowings, or vessel ruptures. CTA is exceptionally sensitive for detecting thrombi and emboli. Magnetic resonance angiography (MRA) is an alternative, especially for patients with iodine contrast allergies or kidney concerns, though it is less commonly available and may have lower resolution for small vessels. These advanced modalities provide the definitive roadmap needed for surgical planning.
Exploratory Surgery: When Imaging Isn't Enough
Sometimes, the diagnosis is made intra-operatively. If a dog presents with acute abdomen and imaging is equivocal or too slow, an exploratory laparotomy (surgical opening of the abdomen) is both diagnostic and therapeutic. The surgeon directly visualizes the intestines and mesentery. Signs of compromised mesenteric ileal branch include: a segment of ileum that is dark purple or black, lacks peristalsis (movement), and feels cooler than adjacent bowel. The mesenteric vessels themselves may be examined for clots or pulsatility. This is the ultimate "look and feel" assessment. If a thrombosis is found in the ileal branch, the surgeon must decide whether to attempt a thrombectomy (clot removal), which is high-risk, or to resect the non-viable bowel and hope collateral flow from the ileocolic or jejunal arteries can compensate for the lost ileal branch.
Surgical Considerations: Preserving a Lifeline
Identifying and Isolating the Vessel
During any surgery involving the caudal small intestine, the first step is meticulous mesenteric dissection. The surgeon must identify the superior mesenteric artery and trace its branches. The mesenteric ileal branch is identified as it courses toward the ileum. Gentle handling with fine instruments is paramount. The vessel is then isolated from surrounding fat and nerves using blunt and sharp dissection. This isolation allows for precise placement of ligatures (sutures used to tie off vessels) or vascular clips. The key principle is to ligate as close to the parent vessel (SMA) as possible to preserve the maximum length of the distal ileal branch and its arcades, ensuring the remaining bowel has the best possible blood supply from whatever collateral sources exist.
Techniques to Minimize Intraoperative Damage
Vessel-sparing techniques are the hallmark of modern veterinary surgery. This includes:
- Using magnification: Surgical loops or microscopes to visualize tiny vessels.
- Gentle tissue handling: Avoiding excessive traction or crushing of the mesentery with forceps.
- Proper ligature placement: Using non-absorbable suture material (like silk) and placing the tie proximal to the intended resection point, but not so close as to risk slipping. A double ligature is often standard for arteries of this size.
- Avoiding thermal injury: Cautery (electrosurgery) is used cautiously near major vessels; ultrasonic scalpels or sharp dissection is preferred.
- Assessing bowel viability: Before finalizing an anastomosis (reconnection), the surgeon uses clinical judgment (color, peristalsis, mesenteric arterial pulsatility) and sometimes intraoperative fluorescence angiography (using a dye like indocyanine green and a special camera) to map blood flow in real-time.
Ligation vs. Preservation: Making the Right Call
The fundamental surgical decision is whether to preserve or ligate the mesenteric ileal branch. Preservation is always the goal when possible. However, if a segment of ileum is diseased (e.g., with a tumor, severe inflammation, or necrosis), that segment and its dedicated blood supply must be removed. The critical decision point is where to ligate the ileal branch. Ligation must occur proximal to the diseased bowel. If the disease is very distal, involving the last few centimeters of ileum, the surgeon might ligate the ileal branch itself and rely on the ileocolic artery to supply the remaining very distal ileum. If the disease is more proximal, the ileal branch may need to be ligated higher up, potentially sacrificing a longer segment of ileum but ensuring the remaining bowel has a robust blood supply from the jejunal arcades. This is a complex judgment call balancing the need for complete disease removal with the imperative to leave enough well-perfused intestine to sustain life.
Post-Operative Care and Monitoring
Signs of Complications to Watch For
After any surgery involving the mesenteric vessels, vigilant monitoring for ischemia or anastomotic leak is critical. Owners should be educated to watch for:
- Lethargy and depression: A dog that seems more tired than expected post-op.
- Persistent or recurrent vomiting: Especially if vomiting becomes bilious (yellow/green) or feculent (smells like stool).
- Abdominal pain: Evidenced by whining, a "praying" position (front legs stretched, rear raised), or guarding when the belly is touched.
- Diarrhea or hematochezia: Bloody diarrhea or stool.
- Fever: A temperature above 103°F (39.4°C).
- Anorexia: Complete refusal to eat beyond the first 24 hours.
These signs, especially in combination, could indicate that a portion of the intestine has lost its blood supply from the mesenteric ileal branch or another vessel, leading to necrosis and potentially fatal peritonitis. Immediate veterinary attention is required.
Medical Management to Support Recovery
Post-operative medical therapy aims to support the remaining bowel and prevent complications. This typically includes:
- Fluid therapy: Aggressive IV fluids to maintain perfusion and correct electrolyte imbalances from vomiting/diarrhea.
- Pain management: Multi-modal analgesia (opioids, NSAIDs, local blocks) is crucial. Pain itself can reduce gut motility.
- Gastroprotectants: Medications like omeprazole or sucralfate to reduce gastric acid and protect the stomach and intestinal lining.
- Antibiotics: Broad-spectrum coverage to prevent or treat translocation of gut bacteria due to a compromised mucosal barrier.
- Anticoagulants/antiplatelets: In cases of documented thrombosis or embolism, drugs like clopidogrel or dalteparin may be used to prevent clot propagation, though this is a delicate balance with surgical bleeding risk.
- Prokinetics: Drugs like metoclopramide or cisapride to encourage intestinal motility once the immediate post-op ileus (temporary paralysis) resolves.
Nutritional Support for Healing Intestines
Nutrition is paramount for healing intestinal tissue. Initially, nothing by mouth (NPO) is required to allow the surgical site to rest. Once motility returns (often signaled by passing gas or stool), a carefully managed diet is introduced. This typically starts with a low-fat, highly digestible prescription diet. Fat slows gastric emptying and can be malabsorbed if the ileum (key for bile acid and fat absorption) is compromised. Small, frequent meals are offered. In severe cases where a dog cannot eat, enteral nutrition via a feeding tube (esophagostomy or jejunostomy tube) is superior to total parenteral nutrition (TPN), as it helps maintain the health of the intestinal mucosa itself. The diet may need to be supplemented with medium-chain triglycerides (MCTs), which are absorbed directly into the portal vein and do not require bile or the usual fat-digestion process, bypassing a potentially struggling ileum.
Prognosis and Long-Term Outlook
Factors Influencing Recovery
The prognosis after an event affecting the mesenteric ileal branch depends on several critical factors:
- Speed of Intervention: Time from onset of ischemia to restoration of blood flow or resection of dead bowel is the single biggest predictor. Every hour counts.
- Extent of Bowel Compromise: How much intestine lost its blood supply? Resection of large segments (>50-60% of total small intestine) risks short bowel syndrome, a condition of severe malabsorption and chronic diarrhea.
- Underlying Cause: A dog with a resectable foreign body and a cleanly ligated ileal branch has a good prognosis. A dog with severe pancreatitis and widespread mesenteric vasculitis has a guarded to poor prognosis due to the systemic illness and risk of recurrent events.
- Patient Factors: Age, overall health, and presence of other diseases (like kidney disease from sepsis) significantly impact recovery.
- Surgical Skill: The precision of the vascular assessment and anastomosis is paramount.
Quality of Life After Vascular Events
Dogs that survive the acute phase of mesenteric ileal branch compromise can have excellent long-term outcomes if a sufficient length of healthy intestine remains. However, some may experience chronic intermittent issues:
- Malabsorption: Especially if a significant length of ileum was removed. This can lead to weight loss, poor coat condition, and vitamin deficiencies (notably B12 and folate, which are absorbed in the ileum).
- Diarrhea: Can be intermittent or persistent due to rapid transit time and maldigestion.
- Dietary Sensitivity: Often require lifelong prescription or homemade highly digestible diets.
- Risk of Adhesions: Scar tissue forming between bowel loops after surgery/inflammation can cause future obstructions.
With dedicated management—including a tailored diet, possible vitamin supplementation, and close monitoring—many dogs adapt well and enjoy a good quality of life. The key is owner compliance with dietary and medication protocols and prompt attention to any recurrence of gastrointestinal upset.
Prevention and Proactive Care
Protecting Your Dog's Abdominal Health
While you cannot prevent all vascular events, proactive care minimizes risks:
- Prevent Trauma: Keep dogs on leashes, secure yards, and supervise interactions to avoid bite wounds and blunt force trauma.
- Manage Cardiac Disease: For dogs with atrial fibrillation or endocarditis, strict adherence to anticoagulation therapy (e.g., clopidogrel) prescribed by your cardiologist is the primary defense against systemic emboli that could lodge in the mesenteric ileal branch.
- Prevent Pancreatitis: Avoid high-fat diets and table scraps. Maintain a healthy weight. For breeds prone to pancreatitis (e.g., Miniature Schnauzers), be extra vigilant.
- Regular Veterinary Check-ups: Early detection of cardiac murmurs, arrhythmias, or systemic illnesses allows for early intervention before a thromboembolic event occurs.
When to Seek Immediate Veterinary Attention
As a dog owner, recognizing the signs of acute abdomen is your most powerful tool. If your dog shows sudden, severe abdominal pain (guarding, crying when touched, "praying" position), profuse vomiting (especially if bloody), diarrhea (especially with blood), lethargy, or collapse, it is a true emergency. Do not wait. These are the classic signs of conditions like intestinal obstruction, pancreatitis, or mesenteric ischemia—all of which can involve the mesenteric ileal branch. Rush to an emergency veterinary hospital. Clearly communicate the symptoms and their onset time. Your quick action is the first and most vital step in saving your dog's life and preserving their intestinal health.
Conclusion: The Unseen Guardian of Digestion
The mesenteric ileal branch dog is far more than a Latin anatomical term; it is a dynamic, essential conduit of life for a significant portion of the canine digestive tract. Its story is one of precise engineering and profound vulnerability. From its origin on the superior mesenteric artery to its terminal capillaries nourishing the ileal villi, this vessel underpins the very process of nutrient absorption that fuels your dog's body. Its clinical significance resonates in every veterinary surgery room and emergency clinic, where its preservation or restoration dictates outcomes. Pathologies like thrombosis, trauma, and vasculitis turn this lifeline into a liability with terrifying speed, demanding rapid, expert intervention.
Understanding this artery empowers you as a pet owner. It transforms vague symptoms of "stomach ache" into potential red flags for intestinal ischemia. It explains why a cardiologist's anticoagulant prescription is crucial for a dog with heart disease. It highlights the incredible skill and precision required in every abdominal surgery. While we hope our dogs never face a crisis involving this vessel, knowledge is the best preparation. It allows you to be a vigilant observer, an effective communicator with your veterinary team, and a proactive advocate for your dog's long, healthy, and happy life. The next time you see your dog enjoying a meal, remember the intricate vascular highway—the mesenteric ileal branch—that makes that simple joy possible.