Hip Adductors Vs Abductors: Your Complete Guide To Hip Muscle Function And Training
Have you ever wondered why your inner thighs feel the burn during certain exercises while the outside of your hips fires up in others? The answer lies in understanding the critical yet often confusing distinction between your hip adductors and abductors. These two opposing muscle groups are fundamental to everything from walking and stabilizing your pelvis to powerful athletic movements, yet they are frequently misunderstood, neglected, or trained incorrectly. Unlocking the secrets of these muscles isn't just for anatomy students or physical therapists—it's essential for anyone looking to move better, prevent injury, and build a stronger, more resilient lower body. This comprehensive guide will dismantle the confusion, providing you with the knowledge to target, strengthen, and protect these vital hip muscles effectively.
The Foundation: Understanding Hip Anatomy and Movement Planes
Before we dive into the "vs." debate, we must establish the basic language of movement. The human body operates in three primary anatomical planes: the sagittal plane (dividing left/right, involved in forward/backward motion like walking), the frontal plane (dividing front/back, involved in side-to-side motion), and the transverse plane (dividing top/bottom, involved in rotation). The terms "adduction" and "abduction" describe movements primarily in the frontal plane.
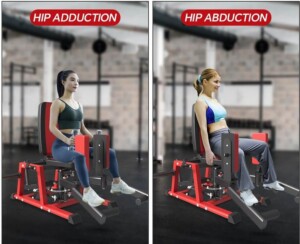
- Adduction refers to movement toward the midline of the body. Imagine bringing your leg from a wide stance back to a neutral position under your hips.
- Abduction refers to movement away from the midline of the body. Think of lifting your leg out to the side, as if creating a "star" shape with your legs.
Understanding this directional opposition is the key to differentiating these muscle groups. They are synergists and antagonists, working in a push-pull relationship to control every lateral motion you make.
Hip Adductors: The Powerful Inner Thigh Muscles
What Are the Hip Adductors?
The hip adductor muscle group is a collection of five primary muscles located on the inner thigh. They originate from the pubis and ischium (the lower, forward part of the hip bone) and insert along the femur (thigh bone). Their collective name comes from their primary action: adduction of the hip. However, their roles are multifaceted and crucial for overall lower body function.
The five major adductors are:
- Adductor Longus: The longest of the group, a primary adductor and weak flexor.
- Adductor Brevis: A shorter, deeper muscle that powerfully adducts and assists in flexion.
- Adductor Magnus: The largest and most powerful adductor. Its posterior fibers also extend the hip, making it a key player in movements like standing up from a chair or climbing.
- Gracilis: A long, thin muscle that adducts but also assists in knee flexion and medial rotation.
- Pectineus: A flat, quadrangular muscle that primarily adducts and flexes the hip.
Primary Functions Beyond Adduction
While adduction is their headline act, these muscles are multitaskers:
- Hip Flexion: The adductor longus, brevis, and pectineus actively help lift the thigh forward.
- Hip Extension: The posterior fibers of the massive adductor magnus are powerful hip extensors, working alongside the gluteus maximus and hamstrings.
- Pelvic Stabilization: This is arguably their most important non-sport-specific role. The adductors, particularly the adductor magnus, form a critical part of the "hip stability tripod" along with the gluteus medius and minimus. They prevent excessive pelvic drop on the opposite side during single-leg stance (like walking), maintaining a level pelvis and efficient gait.
- Medial (Internal) Rotation: Several adductors contribute to rotating the femur inward.
Real-World Importance & Common Dysfunctions
Strong adductors are non-negotiable for:
- Sports: Cutting, pivoting, and changing direction in soccer, basketball, hockey, and tennis.
- Daily Life: Stabilizing yourself when getting in/out of a car, standing on one leg to put on pants, or carrying groceries.
- Injury Prevention: Weak or tight adductors are a primary contributor to groin strains, one of the most common muscle injuries in athletes. They also play a role in knee health, as they help control femur movement, which affects knee tracking. Furthermore, adductor weakness is linked to hip adductor-related groin pain (HAGP) and can contribute to overuse injuries like osteitis pubis.
Hip Abductors: The Crucial Stabilizers of the Hip and Pelvis
What Are the Hip Abductors?
The primary hip abductors are a smaller but incredibly influential group, dominated by the gluteus medius and minimus. The tensor fasciae latae (TFL) is also a significant abductor, though it's often grouped with the IT band complex. Their main action is abduction of the hip, but their stabilizing role is even more critical.
The key abductors are:
- Gluteus Medius: The workhorse. It's the primary hip abductor and the most important stabilizer of the pelvis in the frontal plane during walking and single-leg support.
- Gluteus Minimus: Lies deep to the medius. It's a powerful abductor and medial rotator, assisting the medius in pelvic stabilization.
- Tensor Fasciae Latae (TFL): A smaller muscle on the front of the hip that abducts and medially rotates the femur. It also tensions the iliotibial (IT) band.
Primary Functions: Stability is the Name of the Game
- Pelvic Stabilization (Trendelenburg Sign): This is the abductors' masterpiece. During the single-leg stance phase of walking, the gluteus medius and minimus on the stance leg contract powerfully to prevent the pelvis from dropping on the opposite (swing) side. If these muscles are weak, the pelvis will drop—a sign known as a positive Trendelenburg sign. This inefficient biomechanics leads to a "waddling" gait and places immense stress on the lumbar spine, hip, and knee.
- Hip Abduction: Lifting the leg out to the side, essential for lateral movements.
- Medial (Internal) Rotation: The anterior fibers of the gluteus medius and minimus, along with the TFL, internally rotate the hip.
- Pelvic and Femur Control: They control femoral adduction and internal rotation, which are linked to knee valgus (knees caving in)—a major risk factor for ACL injuries.
Real-World Importance & Common Dysfunctions
Weak abductors, particularly the gluteus medius, are a silent epidemic contributing to:
- Knee Pain (Patellofemoral Pain Syndrome): Poor hip control allows the femur to rotate inward and the knee to cave, increasing stress on the kneecap.
- Low Back Pain: A dropped pelvis on one side forces the lumbar spine into lateral flexion and rotation to compensate, straining muscles and joints.
- IT Band Syndrome: While complex, TFL dominance (often compensating for weak glute med) can increase tension on the IT band, causing friction at the knee.
- Hip Osteoarthritis: Chronic instability and abnormal joint loading from weak abductors may accelerate wear and tear.
Hip Adductors vs Abductors: The Direct Comparison
Now that we've explored each group, let's put them side-by-side to cement the differences.
| Feature | Hip Adductors | Hip Abductors |
|---|---|---|
| Primary Action | Adduction (movement toward midline) | Abduction (movement away from midline) |
| Key Muscles | Adductor Longus, Brevis, Magnus; Gracilis; Pectineus | Gluteus Medius, Minimus; Tensor Fasciae Latae |
| Location | Inner thigh (medial thigh) | Lateral/Posterior hip (gluteal region) |
| Primary Role | Dynamic Power & Multi-joint Movement (flex/extend, stabilize in multiple planes) | Frontal Plane Stability & Pelvic Control (single-leg stance, gait) |
| Critical Function | Generating power for sprinting, kicking, direction change; pelvic stability tripod member | Preventing pelvic drop (Trendelenburg control); controlling femur/knee valgus |
| Common Weakness | Often overlooked in training, leading to groin strains | Extremely common, especially in sedentary individuals and runners, linked to knee/back pain |
| Common Tightness | Very common, especially in athletes, limiting mobility and causing groin pain | TFL is commonly tight/overactive, often compensating for weak glute med |
The Synergy: They are not rivals but partners. Think of the abductors (glute med/min) as the primary stabilizers holding the pelvis level, while the adductors (especially adductor magnus) are powerful movers and secondary stabilizers that assist in that stabilization and provide strength for propulsion. A well-functioning hip requires both groups to be strong, mobile, and neurologically coordinated.
Training the Hip Adductors: From Squeezes to Strength
Training the adductors requires moving beyond the outdated "squeeze a ball" mentality. While isometric squeezes have a place for activation and rehab, we need progressive overload through full ranges of motion.
Key Adductor Exercises
- Copenhagen Adduction: The gold standard. Lying on your side, with the top leg supported on a bench, you lift your bottom leg against resistance. This directly loads the adductors in a shortened position and is highly effective for strength and injury prevention.
- Adductor Machine (Hip Adduction): Use it, but with purpose. Perform slow, controlled reps with a full range of motion. Avoid letting the weight stack drop. It's a good tool for isolating the muscle group.
- Sumo Deadlifts & Wide-Stance Squats: These compound movements place the hips in a position of external rotation and slight adduction, heavily recruiting the adductor magnus, especially in the lockout.
- Lateral Lunges (Side Lunges): A fantastic functional movement. As you lunge to the side, the adductors on the lunging leg eccentrically control the descent and concentrically pull you back to center.
- Pillar Bridges with Adductor Squeeze: A great core-integrated move. In a side-lying or supine position, lift into a bridge while actively squeezing a medicine ball or pillow between your knees.
Adductor Training Tips
- Focus on Eccentrics: The adductors are prone to strains during the lengthening phase (e.g., decelerating the leg in a sprint). Slow, controlled negatives in exercises like the Copenhagen are crucial.
- Don't Neglect Hip Flexion/Extension: Since many adductors are also hip flexors (longus, brevis, pectineus) or extensors (magnus), ensure your program includes balanced hip flexion (e.g., lunges, leg raises) and extension (glute bridges, deadlifts) work.
Training the Hip Abductors: Building a Stable Foundation
Abductor training is non-negotiable for long-term joint health. The focus must be on gluteus medius strength and neuromuscular control.
Key Abductor Exercises
- Side-Lying Leg Lifts: The foundational exercise. Keep the torso stable, lead with the heel, and lift the top leg to about 45 degrees. For a challenge, add ankle weights.
- Clamshells: Excellent for targeting the posterior fibers of the glute medius and minimus. Keep feet together and open the top knee like a clamshell, resisting rotation.
- Banded Walks (Lateral & Monster Walks): Using a resistance band around the ankles or knees, walk laterally while maintaining constant tension. This builds endurance in the glute medius in a functional, weight-bearing position.
- Single-Leg RDLs (Romanian Deadlifts): A premier exercise. Standing on one leg, hinge at the hip while reaching toward the floor. The stance leg's abductors (and entire hip complex) work isometrically to prevent pelvic drop and maintain balance.
- Single-Leg Squats & Step-Ups: Any single-leg, weight-bearing exercise forces the abductors to stabilize. Focus on keeping the knee aligned over the toe, not caving in.
Abductor Training Tips
- Quality Over Quantity: Prioritize perfect form. A few reps with a stable pelvis and no lumbar compensation are worth more than 20 sloppy ones.
- Integrate into Warm-ups: Activate your glute medius before any lower body session with 2-3 sets of banded walks or clamshells.
- Address TFL Dominance: If you feel your IT band/tensor fasciae latae "burning" more than your glutes during abduction work, your glute medius may be underactive. Regress the exercise (e.g., do side-lying lifts instead of standing band walks) and focus on mind-muscle connection.
The Interconnected Web: How Adductor/Abductor Imbalance Affects Your Whole Body
It's a mistake to train these groups in isolation. A weak gluteus medius (abductor) often leads to compensatory overuse and tightness in the TFL and adductors. This creates a vicious cycle: weak abductors allow the femur to adduct and internally rotate, which the adductors then try to control, leading to their fatigue and strain. This imbalance manifests as:
- Knee Valgus: The classic "knees caving in" during squats, jumps, and landings.
- Excessive Foot Pronation: The chain reaction continues down to the foot.
- Low Back Compensations: The spine twists and laterally flexes to maintain balance.
- Performance Plateaus: Inefficient force transfer and energy leaks during powerful movements.
Therefore, assessment is key. Watch for a Trendelenburg sign during a single-leg stance. Observe knee alignment during a bodyweight squat. If your knees cave, you likely have an abductor weakness that needs addressing before heavy adductor or quad training.
Practical Application: Sample Weekly Structure & Injury Prevention
A balanced lower body program must include dedicated and integrated work for both groups.
Sample Weekly Focus:
- Day 1 (Strength): Squats (balanced stance), Single-Leg RDLs, Copenhagen Adductions, Clamshells.
- Day 2 (Power/Speed): Deadlifts, Lateral Lunges, Banded Monster Walks, Plyometrics (with focus on knee alignment).
- Day 3 (Recovery/Activation): Light cardio, extensive stretching/mobility for adductors (butterfly stretch, frog stretch) and abductors (figure-4 stretch, IT band foam rolling), isometric adductor squeezes, glute medius activation drills.
Essential Injury Prevention Strategies:
- Always Warm-Up: Include dynamic movements like leg swings (forward/side-to-side), hip circles, and banded activation.
- Prioritize Mobility: Ensure you have adequate hip internal rotation (for adductor length) and external rotation (for glute function). Use the "90/90" position to assess.
- Progress Gradually: When adding new lateral movement sports (like tennis or pickleball), slowly increase volume to allow adductor tendons to adapt.
- Listen to Your Body: Dull, persistent groin pain is a sign of adductor tendinopathy. Lateral hip pain over the greater trochanter can indicate glute medius tendinopathy. Address these early with targeted rehab, not just rest.
Conclusion: Mastering the Balance for Lifelong Movement
The battle of hip adductors vs abductors is a false dichotomy. They are two sides of the same coin—the coin being a stable, powerful, and resilient hip joint. The adductors are your powerhouse movers and multi-directional stabilizers, critical for strength and athleticism. The abductors, led by the gluteus medius, are your essential pelvic stabilizers, the guardians against knee and back pain.
Neglecting one while overworking the other is a recipe for dysfunction. The path to optimal performance and injury-free movement lies in assessing your personal imbalances and implementing a balanced training strategy that builds strength, control, and endurance in both the adductor and abductor chains. Start by testing your single-leg stance and squat form. Incorporate the key exercises outlined here with a focus on quality. By respecting the distinct yet interdependent roles of these hip muscle groups, you build more than just stronger legs—you build a foundation of stability that supports every step, squat, sprint, and stretch for years to come. Your hips are your body's central hub; it's time to give them the comprehensive care they deserve.